

Estimating the number of UK stroke patients eligible for endovascular thrombectomy
- PMID: 29900409
- PMCID: PMC5992738
- DOI: 10.1177/2396987317733343
Estimating the number of UK stroke patients eligible for endovascular thrombectomy
Abstract
Introduction: Endovascular thrombectomy is a highly effective treatment for acute ischemic stroke due to large arterial occlusion. Routine provision will require major changes in service configuration and workforce. An important first step is to quantify the population of stroke patients that could benefit. We estimated the annual UK population suitable for endovascular thrombectomy using standard or advanced imaging for patient selection.
Patients and methods: Evidence from randomised control trials and national registries was combined to estimate UK stroke incidence and define a decision-tree describing the endovascular thrombectomy eligible population.
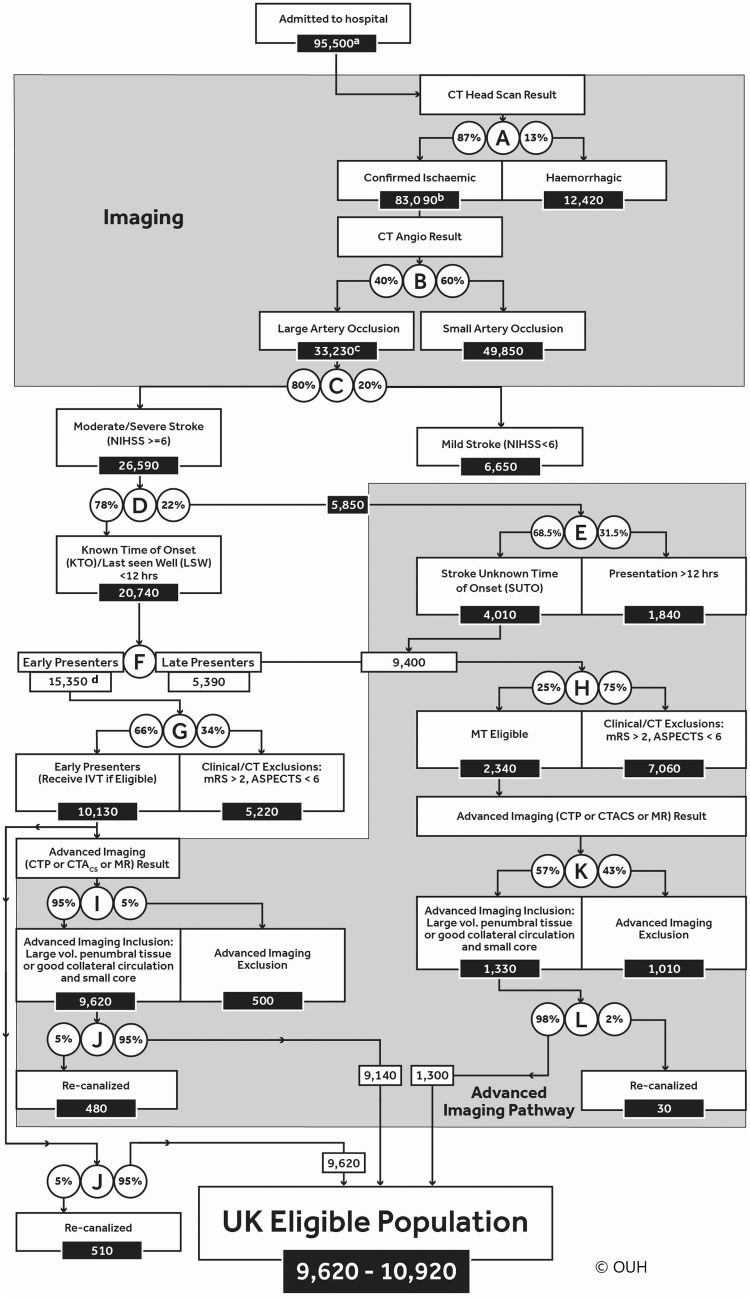
Results: Between 9620 and 10,920 UK stroke patients (approximately 10% of stroke admissions) would be eligible for endovascular thrombectomy annually. The majority (9140-9620) would present within 4 h of onset and be suitable for intravenous thrombolysis. Advanced imaging would exclude 500 patients presenting within 4 h, but identify an additional 1310 patients as eligible who present later.
Discussion: Information from randomised control trials and large registry data provided the evidence criterion for 9 of the 12 decision points. The best available evidence was used for two decision points with sensitivity analyses to determine how key branches of the tree affected estimates. Using the mid-point estimate for eligibility (9.6% of admissions) and assuming national endovascular thrombectomy coverage, 4280 patients would have reduced disability.
Conclusion: A model combining published trials and register data suggests approximately 10% of all stroke admissions in the UK are eligible for endovascular thrombectomy. The use of advanced imaging based on current published evidence did not have a major impact on overall numbers but could alter eligibility status for 16% of cases.
Keywords: Thrombectomy; advanced imaging; ischemic stroke; service planning.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PW is co-PI for two randomised trials (PISTE and STABILISE) investigating different aspects of thrombectomy in acute stroke. Start-up phase of PISTE was mainly funded by Stroke Association but was also part funded by unrestricted institutional educational grants from Covidien and Codman who both manufacture devices used for stroke thrombectomy. STABILISE is part funded by Microvention. PW has also undertaken educational consultancy work within last three years for Codman and Microvention who both manufacture devices used for stroke thrombectomy. GAFs institution has received an educational grant from Medtronic to model thrombectomy need, and honoraria from Pulse Therapeutics for medical advisory work. GAF has received personal remuneration from Medtronic, AstraZeneca, Boehringer Ingelheim, Lundbeck, Cervast, Daiichi Sankyo and Pfizer. MAJ has received personal fees and non-financial support from Boehringer Ingelheim, Bayer, Bristol-Myers-Squibb and Daiichi-Sankyo outside the submitted work.
Figures
References
-
- Berkhemer OA, Puck SS, Fransen PS, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015; 372: 11–20. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 2015; 372: 1009–1018. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 2015; 372: 1019–1030. - PubMed
-
- Saver JL, Goyal M, Bonafe A, et al. Stent-retriever thrombectomy after intravenous t-PA vs t-PA alone in stroke. N Engl J Med 2015; 372: 2285–2295. - PubMed
-
- Jovin TG, Chamorro A, Cobo E, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med 2015; 372: 2296–2306. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
