

Dynamics of virus-specific T cell immunity in pediatric liver transplant recipients
- PMID: 29900673
- PMCID: PMC6117219
- DOI: 10.1111/ajt.14967
Dynamics of virus-specific T cell immunity in pediatric liver transplant recipients
Abstract
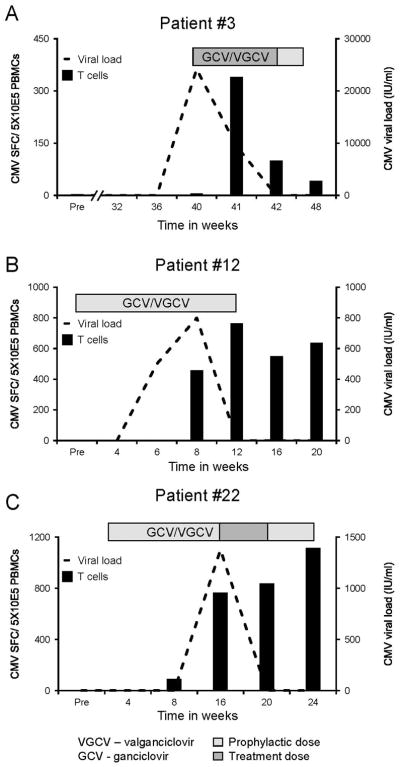
Immunosuppression following solid organ transplantation (SOT) has a deleterious effect on cellular immunity leading to frequent and prolonged viral infections. To better understand the relationship between posttransplant immunosuppression and circulating virus-specific T cells, we prospectively monitored the frequency and function of T cells directed to a range of latent (CMV, EBV, HHV6, BK) and lytic (AdV) viruses in 16 children undergoing liver transplantation for up to 1 year posttransplant. Following transplant, there was an immediate decline in circulating virus-specific T cells, which recovered posttransplant, coincident with the introduction and subsequent routine tapering of immunosuppression. Furthermore, 12 of 14 infections/reactivations that occurred posttransplant were successfully controlled with immunosuppression reduction (and/or antiviral use) and in all cases we detected a temporal increase in the circulating frequency of virus-specific T cells directed against the infecting virus, which was absent in 2 cases where infections remained uncontrolled by the end of follow-up. Our study illustrates the dynamic changes in virus-specific T cells that occur in children following liver transplantation, driven both by active viral replication and modulation of immunosuppression.
Keywords: T cell biology; clinical research/practice; infectious disease; liver transplantation/hepatology; monitoring: immune.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures





References
-
- Toledo-Pereyra LH, Toledo AH. J Invest Surg. 2005;18(6):285–90. 1954. - PubMed
-
- Rana A, Gruessner A, Agopian VG, Khalpey Z, Riaz IB, Kaplan B, et al. Survival benefit of solid-organ transplant in the United States. JAMA Surg. 2015;150(3):252–9. - PubMed
-
- Gonwa TA. Transplantation. Am J Kidney Dis. 2000;35(4 Suppl 1):S153–9. - PubMed
-
- Lodhi SA, Lamb KE, Meier-Kriesche HU. Solid organ allograft survival improvement in the United States: the long-term does not mirror the dramatic short-term success. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2011;11(6):1226–35. - PubMed
-
- LaRosa C, Baluarte HJ, Meyers KE. Outcomes in pediatric solid-organ transplantation. Pediatric transplantation. 2011;15(2):128–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
