

Adult-onset renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion: 3 case reports and review of literature
- PMID: 29901594
- PMCID: PMC6024875
- DOI: 10.1097/MD.0000000000011023
Adult-onset renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion: 3 case reports and review of literature
Abstract
Rationale: Renal cell carcinoma associated with Xp11.2 translocations/TFE3 gene fusions is a rare subtype of renal cell carcinoma. This predominantly occurs in juveniles, but rarely seen in adults with lymph node or organic metastasis and a worsened prognosis.
Patients concerns: Herein, we presented 3 adult cases of Xp11-RCC. Two patients were in early stage and good condition, and the third patient had lymph node metastasis but showed no recurrence after a 3-month follow-up.
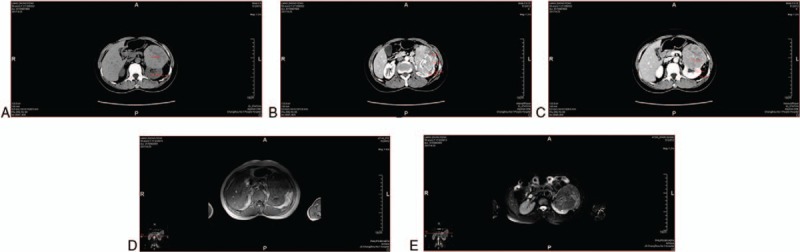
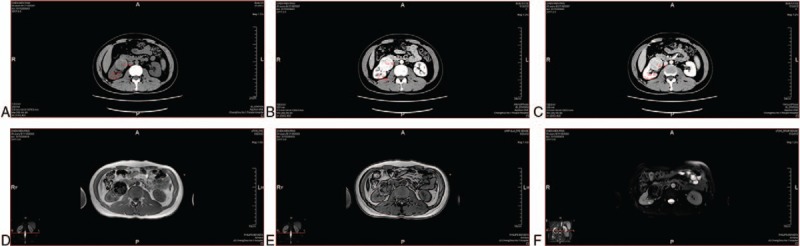
Diagnoses: Case 1: A 50-year-old female without any lumbago and gross hematuria was incidentally detected by left renal mass by ultrasonography. Case 2: A 31-year-old female with 2-year hemodialysis was detected with right renal carcinoma during preoperative examination of renal transplant. Case 3: A 45-year-old male with right lumbago for 1 month was detected with a mass in the lower pole of right kidney by ultrasonography.
Intervention: The characteristics of these 3 images are not consistent with each other, and showed some differences with the previous ones.
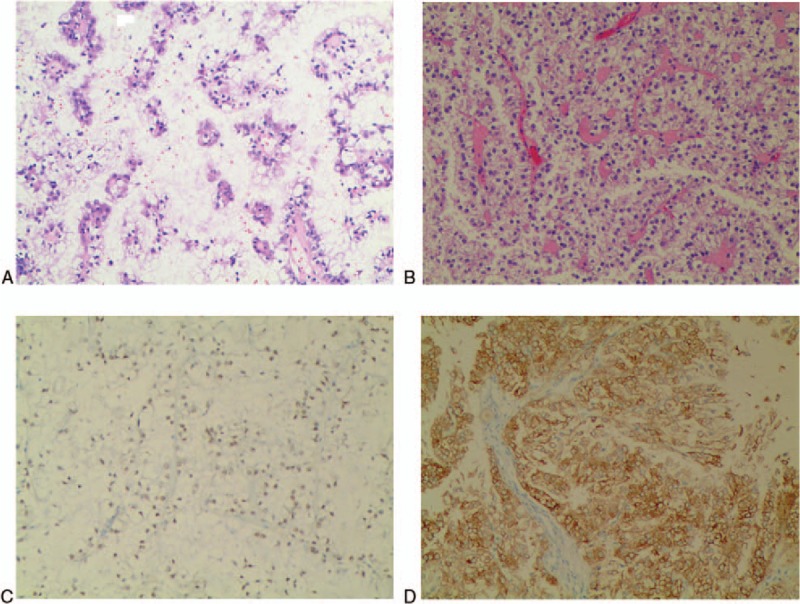
Outcomes: All these 3 patients underwent laparoscopic radical nephrectomy, and case 1 patient underwent renal hilar lymphnode dissection at the same time. Immunohistochemistry was performed on all the 3 tumors, revealing that the tumor cells were positive for TFE3 and Melan-A. Case 1 showed lymph node metastasis, and received mTOR inhibitors. The 3 patients had no recurrent and new metastasis in other organs after follow-up for 3 months, 2 months, and 11 months, respectively.
Lessons: Whether the adult-onset Xp-RCC has an aggressive clinical course still remains controversial. Characteristics of the images of the 3 adult cases showed some uniformity but still have some differences. Immunohistochemistry results revealed tumor cell positive for TFE3, but have no consistency in carbonic anhydrase IX, CD117, Ki67, CK8/18 AE1/AE3 and so on. Therefore, the uniform and definitive diagnostic standards of the tumors are uncertain. Hence, more cases and findings are required to elaborate the standards of all the tumor subtypes. Vascular endothelial growth factor-targeted therapy showed some efficacious results in patients with metastasis, but more useful treatments are warranted.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Xp11 translocation renal cell carcinoma and clear cell renal cell carcinoma with TFE3 strong positive immunostaining: morphology, immunohistochemistry, and FISH analysis.Mod Pathol. 2019 Oct;32(10):1521-1535. doi: 10.1038/s41379-019-0283-z. Epub 2019 Jun 7. Mod Pathol. 2019. PMID: 31175325
-
ALK rearrangement in TFE3-positive renal cell carcinoma: Alternative diagnostic option to exclude Xp11.2 translocation carcinoma.Pathol Res Pract. 2020 Dec;216(12):153286. doi: 10.1016/j.prp.2020.153286. Epub 2020 Nov 9. Pathol Res Pract. 2020. PMID: 33197836 Review.
-
Renal Cell Carcinoma Associated with Xp11.2 Translocation/TFE3 Gene Fusions: Clinical Features, Treatments and Prognosis.PLoS One. 2016 Nov 28;11(11):e0166897. doi: 10.1371/journal.pone.0166897. eCollection 2016. PLoS One. 2016. PMID: 27893792 Free PMC article.
-
A case of PSF-TFE3 gene fusion in Xp11.2 renal cell carcinoma with melanotic features.Hum Pathol. 2015 Mar;46(3):476-81. doi: 10.1016/j.humpath.2014.11.013. Epub 2014 Dec 9. Hum Pathol. 2015. PMID: 25582502
-
Clinical heterogeneity of Xp11 translocation renal cell carcinoma: impact of fusion subtype, age, and stage.Mod Pathol. 2014 Jun;27(6):875-86. doi: 10.1038/modpathol.2013.208. Epub 2013 Dec 6. Mod Pathol. 2014. PMID: 24309327 Review.
Cited by
-
The Latinx Disparity in Surgery for Kidney Cancer: Data from The South Texas Region.Kidney Cancer J. 2022 Mar;20(1):6-13. doi: 10.52733/KCJ20n1-a1. Epub 2022 Mar 17. Kidney Cancer J. 2022. PMID: 35646227 Free PMC article.
-
Factors Associated with Survival From Xp11.2 Translocation Renal Cell Carcinoma Diagnosis-A Systematic Review and Pooled Analysis.Pathol Oncol Res. 2021 Mar 30;27:610360. doi: 10.3389/pore.2021.610360. eCollection 2021. Pathol Oncol Res. 2021. PMID: 34257577 Free PMC article.
-
MRI Characteristics of Pediatric and Young-Adult Renal Cell Carcinoma: A Single-Center Retrospective Study and Literature Review.Cancers (Basel). 2023 Feb 22;15(5):1401. doi: 10.3390/cancers15051401. Cancers (Basel). 2023. PMID: 36900194 Free PMC article. Review.
-
Multimodality imaging of Xp11.2 translocation/TFE3 gene fusion associated with renal cell carcinoma: a case report.Front Med (Lausanne). 2023 Sep 19;10:1266630. doi: 10.3389/fmed.2023.1266630. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37795411 Free PMC article.
References
-
- Lopez-Beltran A, Scarpelli M, Montironi R, et al. 2004 WHO classification of the renal tumors of the adults. Eur Urol 2006;49:798–805. - PubMed
-
- Bruder E, Passera O, Harms D, et al. Morphologic and molecular characterization of renal cell carcinoma in children and young adults. Am J Surg Pathol 2004;28:1117–32. - PubMed
-
- Argani P, Olgac S, Tickoo SK, et al. Xp11 translocation renal cell carcinoma in adults: expanded clinical, pathologic, and genetic spectrum. Am J Surg Pathol 2007;31:1149–60. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
