

The effects of preoperative single-dose thoracic paravertebral block on acute and chronic pain after thoracotomy: A randomized, controlled, double-blind trial
- PMID: 29901652
- PMCID: PMC6023649
- DOI: 10.1097/MD.0000000000011181
The effects of preoperative single-dose thoracic paravertebral block on acute and chronic pain after thoracotomy: A randomized, controlled, double-blind trial
Abstract
Background: Patients undergoing thoracotomy frequently experience acute pain and chronic post-thoracotomy pain (CPTP). There are few articles relating to the investigations on the effects of preoperative single-dose thoracic paravertebral block (PSTPVB) on acute pain and CPTP. We tested the hypothesis that adding PSTPVB to intravenous (IV) patient-controlled analgesia (PCA) would reduce acute pain scores and decrease the incidence and intensity of CPTP.
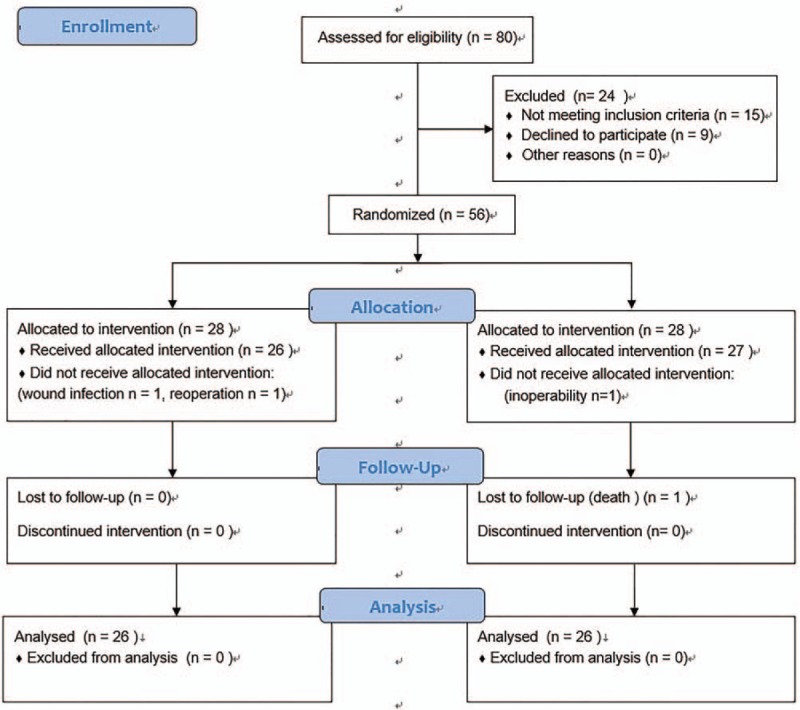
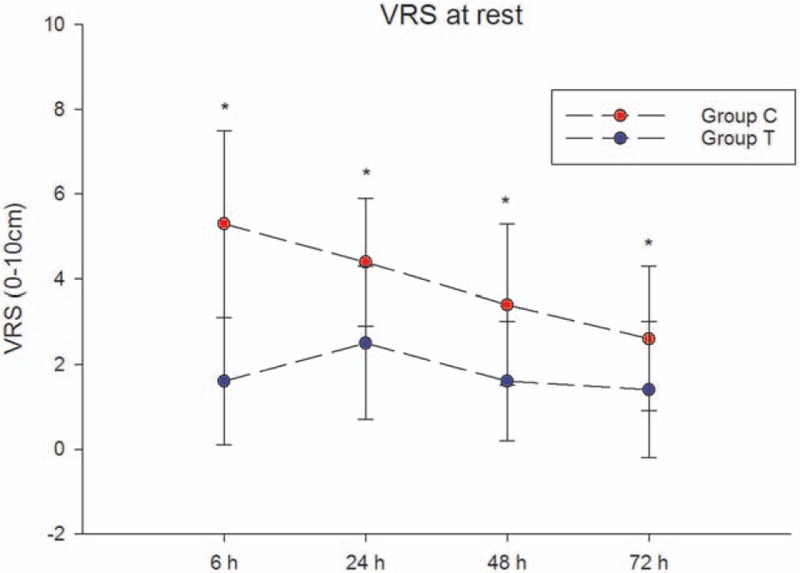
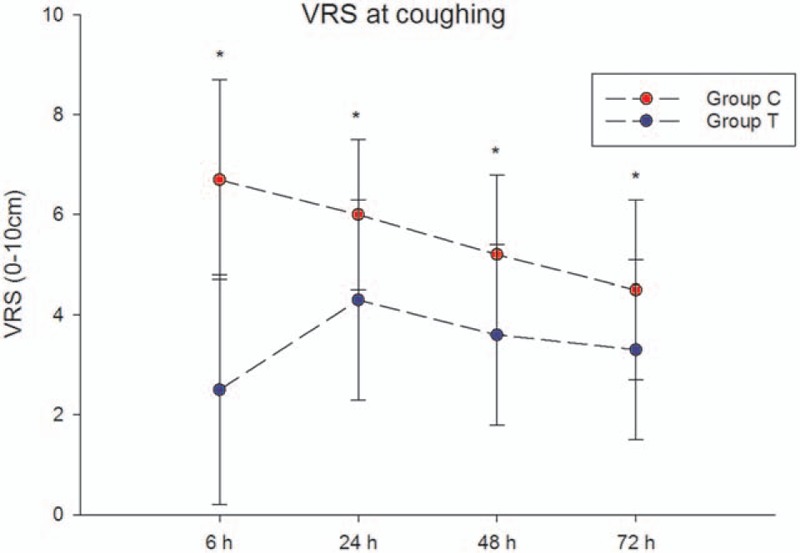
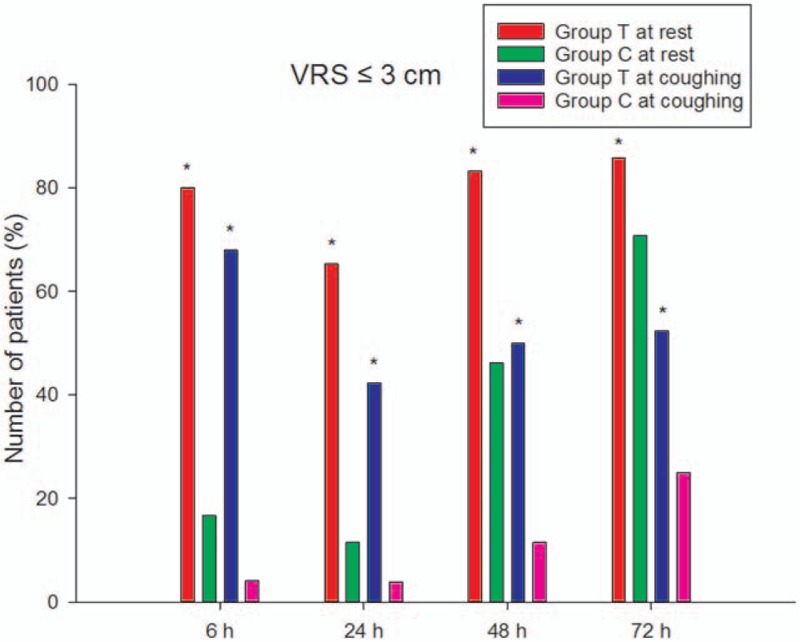
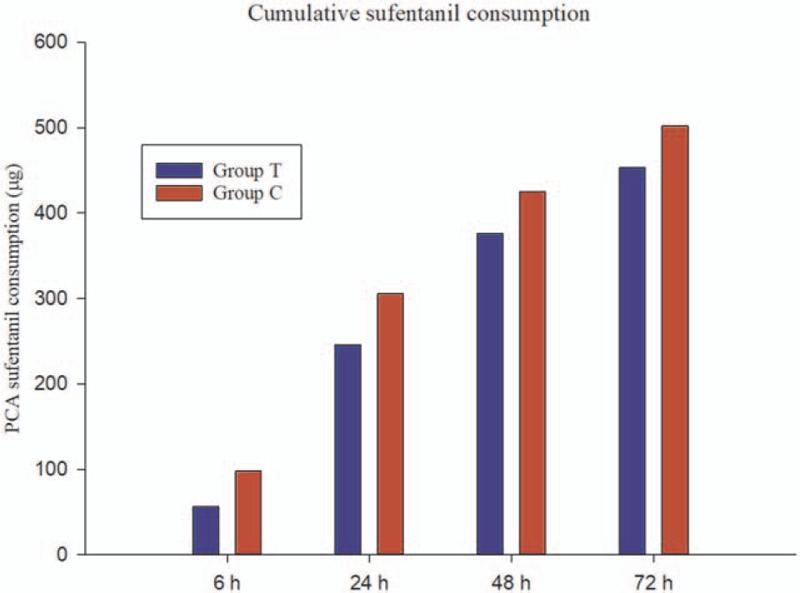
Methods: Fifty-six patients undergoing elective thoracotomy were randomized to receive PSTPVB in addition to IV PCA (group T) or IV PCA alone (group C). A single 20-mL injection of 0.50% ropivacaine plus 10 mg dexamethasone in saline was administered preoperatively under ultrasound guidance; sufentanil was used for IV PCA. The acute pain intensity at rest and at coughing based on verbal rating scale, postoperative sufentanil consumption, and complications were evaluated at 6, 24, 48, and 72 hours after surgery. The incidence and intensity of CPTP were evaluated at 3 months after surgery.
Results: Group T had significantly less acute pain compared with group C at all measurement times both at rest and at coughing (P < .05). The PCA cumulative sufentanil consumption, complications, and the incidence of CPTP between the 2 groups was not statistically significant (P > .05). The intensity of CPTP was significantly higher in group C than in group T (P < .05).
Conclusion: This study indicated that adding PSTPVB to IV PCA improved acute postoperative pain and chronic pain in patients undergoing thoracotomy, but did not reduce the incidence of CPTP.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Single-dose, bilateral paravertebral block plus intravenous sufentanil analgesia in patients with esophageal cancer undergoing combined thoracoscopic-laparoscopic esophagectomy: a safe and effective alternative.J Cardiothorac Vasc Anesth. 2014 Aug;28(4):966-72. doi: 10.1053/j.jvca.2013.12.007. Epub 2014 Mar 29. J Cardiothorac Vasc Anesth. 2014. PMID: 24686029 Clinical Trial.
-
Continuous right thoracic paravertebral block following bolus initiation reduced postoperative pain after right-lobe hepatectomy: a randomized, double-blind, placebo-controlled trial.Reg Anesth Pain Med. 2014 Nov-Dec;39(6):506-12. doi: 10.1097/AAP.0000000000000167. Reg Anesth Pain Med. 2014. PMID: 25304475 Free PMC article. Clinical Trial.
-
Chronic postthoracotomy pain and perioperative ketamine infusion.J Pain Palliat Care Pharmacother. 2014 Jun;28(2):117-21. doi: 10.3109/15360288.2014.908992. Epub 2014 May 6. J Pain Palliat Care Pharmacother. 2014. PMID: 24799159 Clinical Trial.
-
Intra-operative paravertebral block for postoperative analgesia in thoracotomy patients: a randomized, double-blind, placebo-controlled study.Eur J Cardiothorac Surg. 2011 Oct;40(4):902-6. doi: 10.1016/j.ejcts.2011.01.067. Epub 2011 Mar 5. Eur J Cardiothorac Surg. 2011. PMID: 21377888 Review.
-
Hydromorphone vs sufentanil in patient-controlled analgesia for postoperative pain management: A meta-analysis.Medicine (Baltimore). 2022 Jan 21;101(3):e28615. doi: 10.1097/MD.0000000000028615. Medicine (Baltimore). 2022. PMID: 35060534 Free PMC article.
Cited by
-
Thoracic Paravertebral Blockade Reduces Chronic Postsurgical Pain in Breast Cancer Patients: A Randomized Controlled Trial.Pain Med. 2020 Dec 25;21(12):3539-3547. doi: 10.1093/pm/pnaa270. Pain Med. 2020. PMID: 33111950 Free PMC article. Clinical Trial.
-
Improved Analgesic Effect of Paravertebral Blocks before and after Video-Assisted Thoracic Surgery: A Prospective, Double-Blinded, Randomized Controlled Trial.Pain Res Manag. 2019 Nov 18;2019:9158653. doi: 10.1155/2019/9158653. eCollection 2019. Pain Res Manag. 2019. PMID: 31827657 Free PMC article. Clinical Trial.
-
Pain management after thoracotomy with dexamethasone and bupivacaine through a peripleural cather: a randomized controlled trial.BMC Anesthesiol. 2024 Jul 16;24(1):240. doi: 10.1186/s12871-024-02625-3. BMC Anesthesiol. 2024. PMID: 39014323 Free PMC article. Clinical Trial.
-
Comparison of tracheal intubation with controlled ventilation and laryngeal mask airway with spontaneous ventilation for thoracoscopic bullectomy.Medicine (Baltimore). 2020 Apr;99(16):e19704. doi: 10.1097/MD.0000000000019704. Medicine (Baltimore). 2020. PMID: 32311952 Free PMC article.
-
The role of regional anaesthesia and multimodal analgesia in the prevention of chronic postoperative pain: a narrative review.Anaesthesia. 2021 Jan;76 Suppl 1(Suppl 1):8-17. doi: 10.1111/anae.15256. Anaesthesia. 2021. PMID: 33426669 Free PMC article. Review.
References
-
- Kavanagh BP, Katz J, Sandler AN. Pain control after thoracic surgery. A review of current techniques. Anesthesiology 1994;81:737–59. - PubMed
-
- Baik JS, Oh AY, Cho CW, et al. Thoracic paravertebral block for nephrectomy: a randomized, controlled, observer-blinded study. Pain Med 2014;15:850–6. - PubMed
-
- Sabanathan S, Mearns AJ, Bickford SP, et al. Efficacy of continuous extrapleural intercostal nerve block on post-thoracotomy pain and pulmonary mechanics. Br J Surg 1990;77:221–5. - PubMed
-
- Wildgaard K, Ravn J, Kehlet H. Chronic post-thoracotomy pain: a critical review of pathogenic mechanisms and strategies for prevention. Eur J Cardiothorac Surg 2009;36:170–80. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
