

Circulating cotinine concentrations and lung cancer risk in the Lung Cancer Cohort Consortium (LC3)
- PMID: 29901778
- PMCID: PMC6280953
- DOI: 10.1093/ije/dyy100
Circulating cotinine concentrations and lung cancer risk in the Lung Cancer Cohort Consortium (LC3)
Abstract
Background: Self-reported smoking is the principal measure used to assess lung cancer risk in epidemiological studies. We evaluated if circulating cotinine-a nicotine metabolite and biomarker of recent tobacco exposure-provides additional information on lung cancer risk.
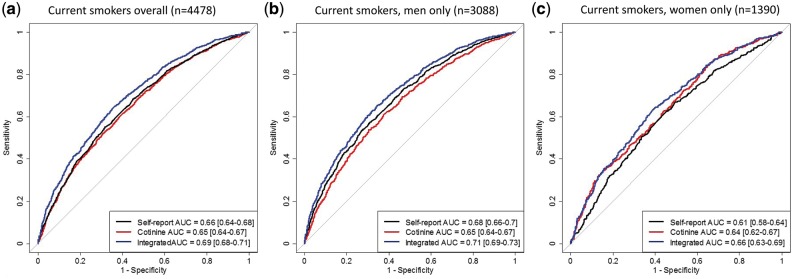
Methods: The study was conducted in the Lung Cancer Cohort Consortium (LC3) involving 20 prospective cohort studies. Pre-diagnostic serum cotinine concentrations were measured in one laboratory on 5364 lung cancer cases and 5364 individually matched controls. We used conditional logistic regression to evaluate the association between circulating cotinine and lung cancer, and assessed if cotinine provided additional risk-discriminative information compared with self-reported smoking (smoking status, smoking intensity, smoking duration), using receiver-operating characteristic (ROC) curve analysis.
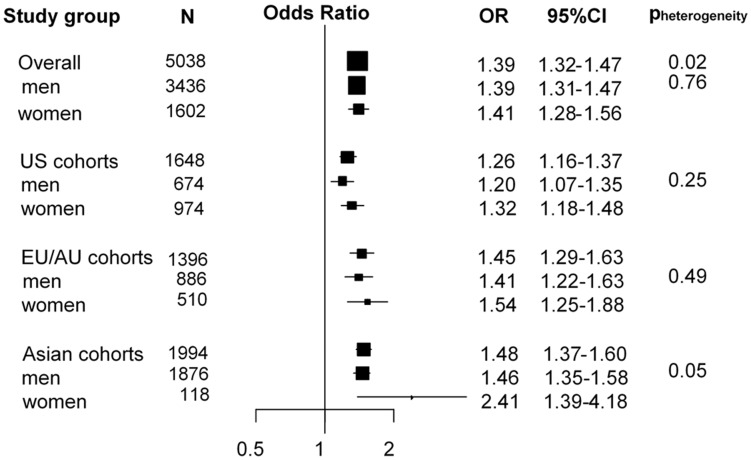
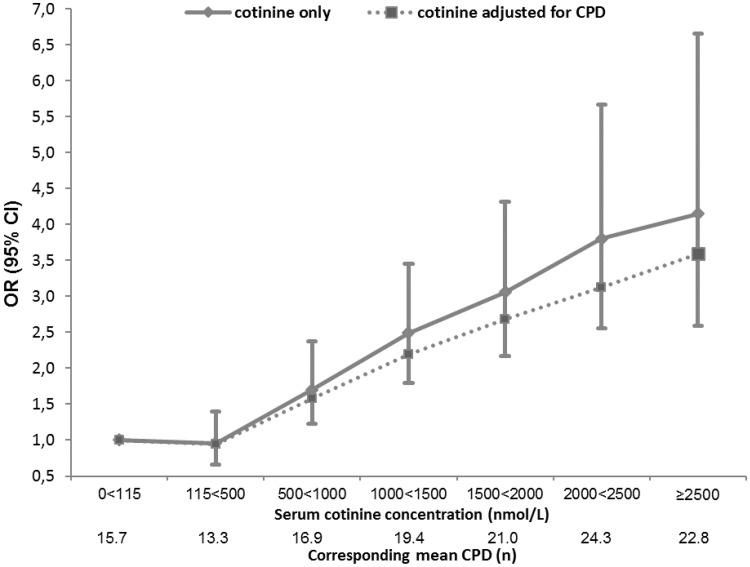
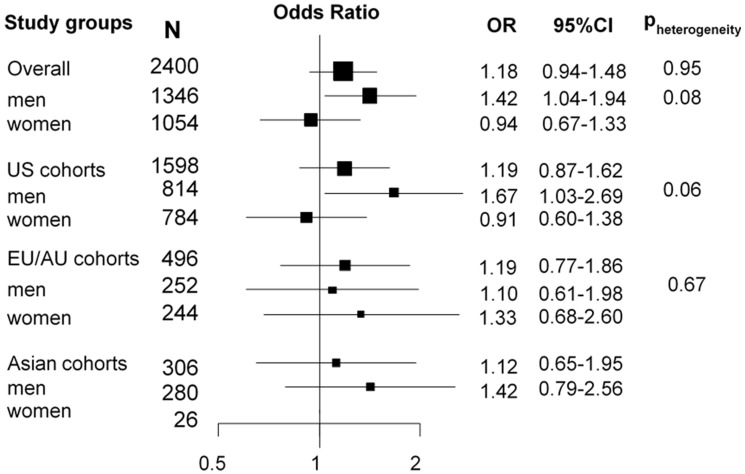
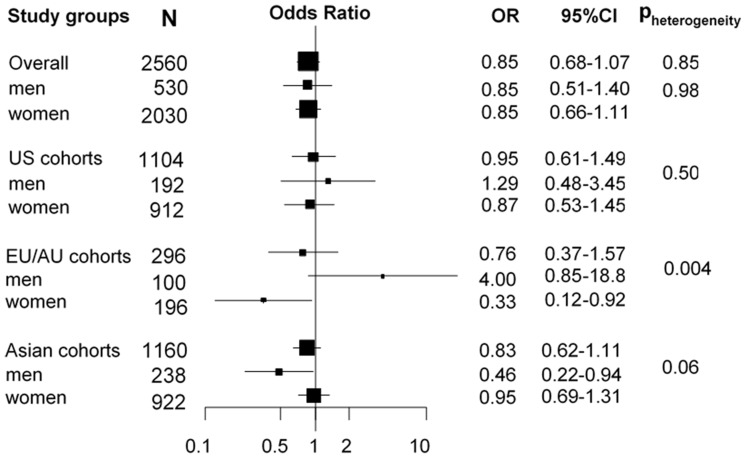
Results: We observed a strong positive association between cotinine and lung cancer risk for current smokers [odds ratio (OR ) per 500 nmol/L increase in cotinine (OR500): 1.39, 95% confidence interval (CI): 1.32-1.47]. Cotinine concentrations consistent with active smoking (≥115 nmol/L) were common in former smokers (cases: 14.6%; controls: 9.2%) and rare in never smokers (cases: 2.7%; controls: 0.8%). Former and never smokers with cotinine concentrations indicative of active smoking (≥115 nmol/L) also showed increased lung cancer risk. For current smokers, the risk-discriminative performance of cotinine combined with self-reported smoking (AUCintegrated: 0.69, 95% CI: 0.68-0.71) yielded a small improvement over self-reported smoking alone (AUCsmoke: 0.66, 95% CI: 0.64-0.68) (P = 1.5x10-9).
Conclusions: Circulating cotinine concentrations are consistently associated with lung cancer risk for current smokers and provide additional risk-discriminative information compared with self-report smoking alone.
Figures
References
-
- World Health Organization. Cancer Fact Sheet 2017 http://www.who.int/mediacentre/factsheets/fs297/en/ (February 2017, date last accessed).
-
- Stewart BW, Wild CP (eds). World Cancer Report 2014 Lyon, France: International Agency for Research on Cancer, 2014. - PubMed
-
- Malhotra J, Malvezzi M, Negri E, La Vecchia C, Boffetta P.. Risk factors for lung cancer worldwide. Eur Respir J 2016;48:889–902. - PubMed
-
- Corbin M, Haslett S, Pearce N, Maule M, Greenland S.. A comparison of sensitivity-specificity imputation, direct imputation and fully Bayesian analysis to adjust for exposure misclassification when validation data are unavailable. Int J Epidemiol 2017;46:1063–72. - PubMed
-
- Benowitz NL, Jacob P 3rd.. Metabolism of nicotine to cotinine studied by a dual stable isotope method. Clin Pharmacol Ther 1994;56:483–93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201600001C/HL/NHLBI NIH HHS/United States
- HHSN268201600003C/HL/NHLBI NIH HHS/United States
- R01 CA049449/CA/NCI NIH HHS/United States
- P01 CA087969/CA/NCI NIH HHS/United States
- P30 ES006694/ES/NIEHS NIH HHS/United States
- U01 CA182876/CA/NCI NIH HHS/United States
- HHSN268201600002C/HL/NHLBI NIH HHS/United States
- HHSN268201600004C/HL/NHLBI NIH HHS/United States
- HHSN268201600018C/HL/NHLBI NIH HHS/United States
- UM1 CA167552/CA/NCI NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- U01 CA155340/CA/NCI NIH HHS/United States
- UM1 CA182876/CA/NCI NIH HHS/United States
- R01 CA144034/CA/NCI NIH HHS/United States
- UM1 CA182934/CA/NCI NIH HHS/United States
- P50 CA127003/CA/NCI NIH HHS/United States
- RC1 HL099355/HL/NHLBI NIH HHS/United States
- P30 CA071789/CA/NCI NIH HHS/United States
- 001/WHO_/World Health Organization/International
- U01 CA164973/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
