

Congenital Hyperinsulinism in Infants with Turner Syndrome: Possible Association with Monosomy X and KDM6A Haploinsufficiency
- PMID: 29902804
- PMCID: PMC6067979
- DOI: 10.1159/000488347
Congenital Hyperinsulinism in Infants with Turner Syndrome: Possible Association with Monosomy X and KDM6A Haploinsufficiency
Abstract
Background: Previous case reports have suggested a possible association of congenital hyperinsulinism with Turner syndrome.
Objective: We examined the clinical and molecular features in girls with both congenital hyperinsulinism and Turner syndrome seen at The Children's Hospital of Philadelphia (CHOP) between 1974 and 2017.
Methods: Records of girls with hyperinsulinism and Turner syndrome were reviewed. Insulin secretion was studied in pancreatic islets and in mouse islets treated with an inhibitor of KDM6A, an X chromosome gene associated with hyperinsulinism in Kabuki syndrome.
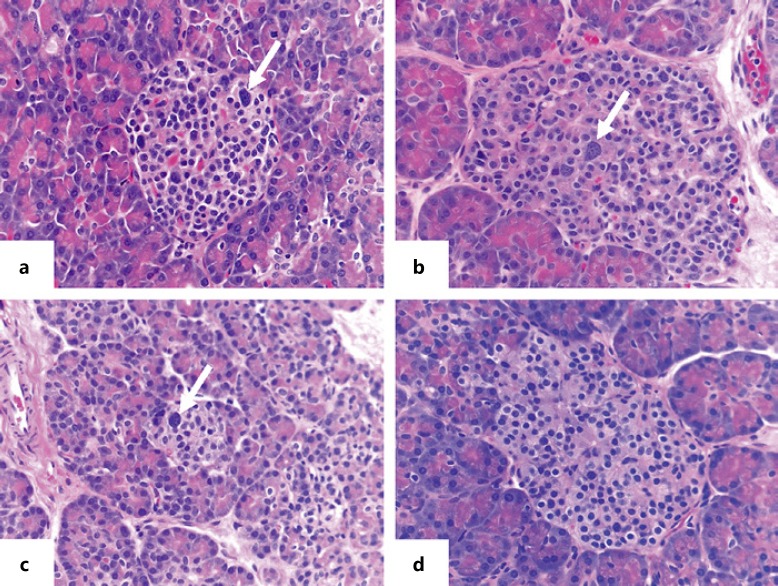
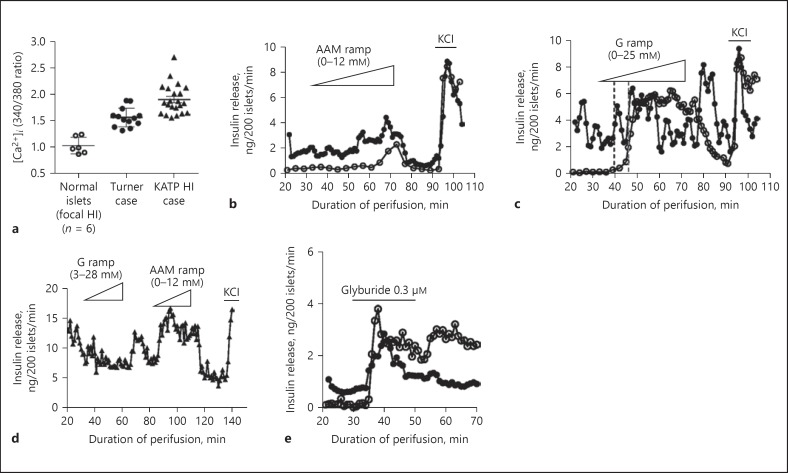
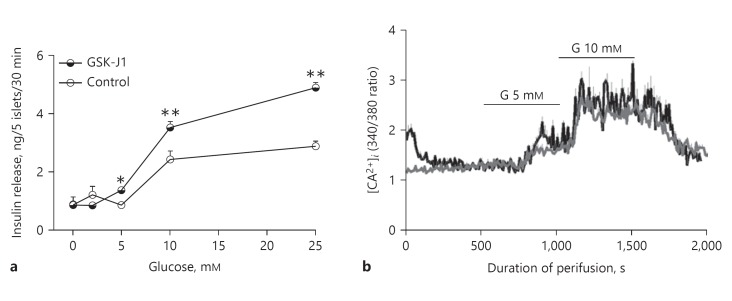
Results: Hyperinsulinism was diagnosed in 12 girls with Turner syndrome. Six were diazoxide-unresponsive; 3 had pancreatectomies. The incidence of Turner syndrome among CHOP patients with hyperinsulinism (10 of 1,050 from 1997 to 2017) was 48 times more frequent than expected. The only consistent chromosomal anomaly in these girls was the presence of a 45,X cell line. Studies of isolated islets from 1 case showed abnormal elevated cytosolic calcium and heightened sensitivity to amino acid-stimulated insulin release; similar alterations were demonstrated in mouse islets treated with a KDM6A inhibitor.
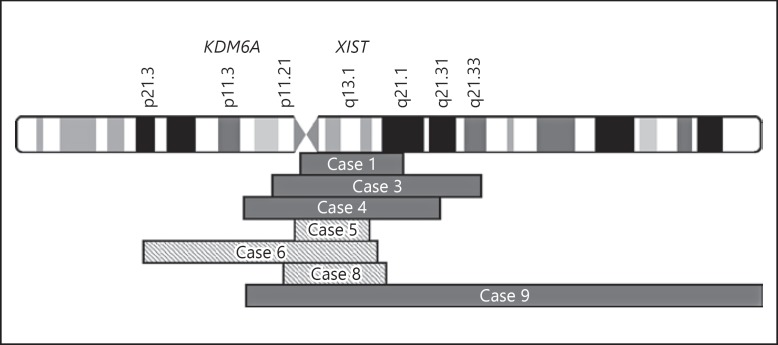
Conclusion: These results demonstrate a higher than expected frequency of Turner syndrome among children with hyperinsulinism. Our data suggest that haploinsufficiency for KDM6A due to mosaic X chromosome monosomy may be responsible for hyperinsulinism in Turner syndrome.
Keywords: Beta cell; Congenital hyperinsulinism; Diazoxide; Genetics; Hypoglycemia; Pancreatectomy; Turner syndrome; X chromosome.
The Author(s). Published by S. Karger AG, Basel.
Figures
References
-
- Bondy CA, Turner Syndrome Study Group Care of girls and women with Turner syndrome: a guideline of the Turner Syndrome Study Group. J Clin Endocrinol Metab. 2007 Jan;92((1)):10–25. - PubMed
-
- Gravholt CH, Andersen NH, Conway GS, Dekkers OM, Geffner ME, Klein KO, et al. International Turner Syndrome Consensus Group Clinical practice guidelines for the care of girls and women with Turner syndrome: proceedings from the 2016 Cincinnati International Turner Syndrome Meeting. Eur J Endocrinol. 2017 Sep;177((3)):G1–70. - PubMed
-
- Nielsen J, Wohlert M. Chromosome abnormalities found among 34,910 newborn children: results from a 13-year incidence study in Arhus, Denmark. Hum Genet. 1991 May;87((1)):81–3. - PubMed
-
- Bakalov VK, Cooley MM, Quon MJ, Luo ML, Yanovski JA, Nelson LM, et al. Impaired insulin secretion in the Turner metabolic syndrome. J Clin Endocrinol Metab. 2004 Jul;89((7)):3516–20. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
