

Severely impaired terminal erythroid differentiation as an independent prognostic marker in myelodysplastic syndromes
- PMID: 29903708
- PMCID: PMC6020814
- DOI: 10.1182/bloodadvances.2018018440
Severely impaired terminal erythroid differentiation as an independent prognostic marker in myelodysplastic syndromes
Abstract
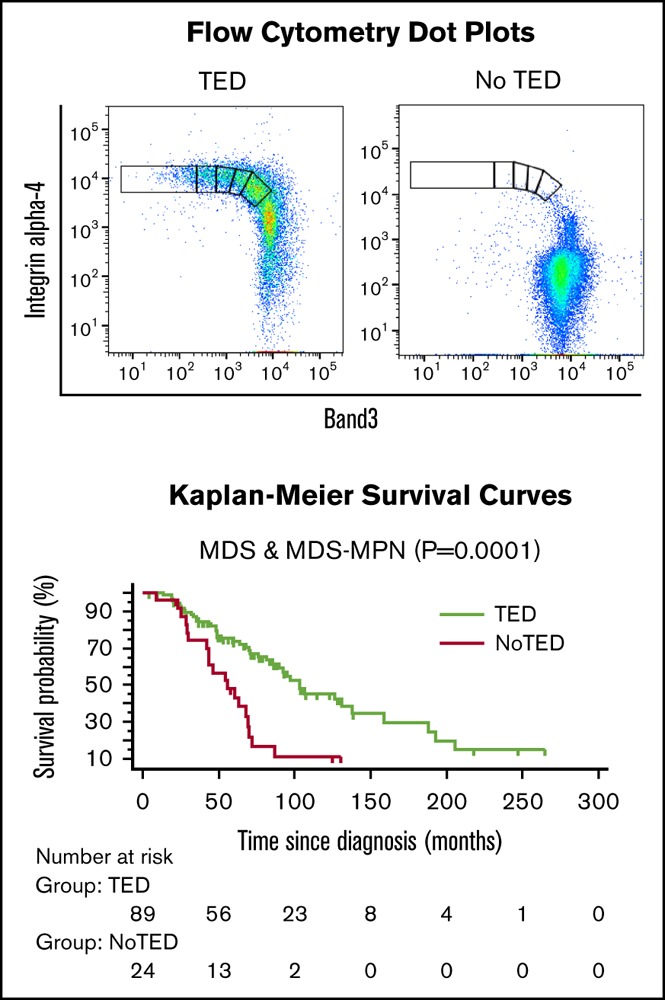
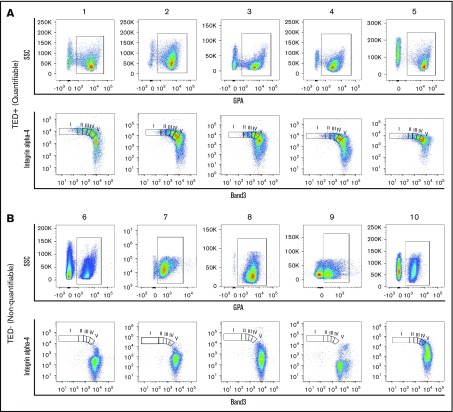
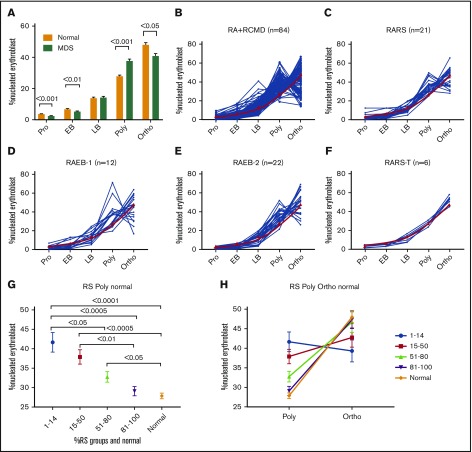
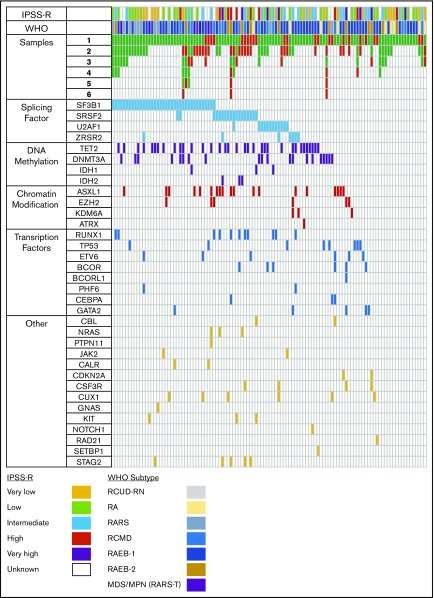
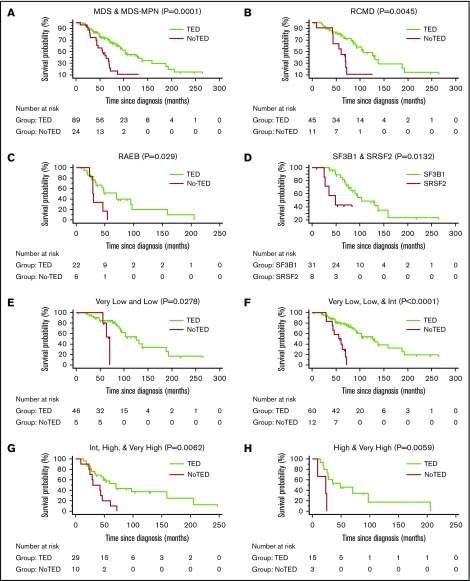
Anemia is the defining feature in most patients with myelodysplastic syndromes (MDS), yet defects in erythropoiesis have not been well characterized. We examined freshly obtained bone marrow (BM) samples for stage-specific abnormalities during terminal erythroid differentiation (TED) from 221 samples (MDS, n = 205 from 113 unique patients; normal, n = 16) by measuring the surface expression of glycophorin A, band 3, and integrin α-4. Clinical and biologic associations were sought with presence or absence of TED and the specific stage of erythroid arrest. In 27% of MDS samples (56/205), there was no quantifiable TED documented by surface expression of integrin α-4 and band 3 by terminally differentiating erythroblasts. Absence of quantifiable TED was associated with a significantly worse overall survival (56 vs 103 months, P = .0001) and SRSF2 mutations (7/23, P < .05). In a multivariable Cox proportional hazards regression analysis, absence of TED remained independently significant across International Prognostic Scoring System-Revised (IPSS-R) categories, myeloid/erythroid ratio, and mutations in several genes. In 149/205 MDS samples, the proportion of cells undergoing TED did not follow the expected 1:2:4:8:16 doubling pattern in successive stages. Absence of TED emerged as a powerful independent prognostic marker of poor overall survival across all IPSS-R categories in MDS, and SRSF2 mutations were more frequently associated with absence of TED.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Raza A, Galili N. The genetic basis of phenotypic heterogeneity in myelodysplastic syndromes. Nat Rev Cancer. 2012;12(12):849-859. - PubMed
-
- Pomares H, Sánchez-Ortega I, Alonso E, et al. . Validation of the Low Risk Prognostic Scoring System (LR-PSS) in patients with very low, low and intermediate risk IPSS-R myelodysplastic syndrome. Results from a single center. Blood. 2015;126(23):2902.
-
- Shiozawa Y, Malcovati L, Gallì A, et al. . Gene expression and risk of leukemic transformation in myelodysplasia. Blood. 2017;130(24):2642-2653. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
