

Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS
- PMID: 29903755
- PMCID: PMC6410734
- DOI: 10.1136/thoraxjnl-2017-211280
Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS
Abstract
Background: There is no accurate, non-invasive measurement to estimate the degree of pulmonary oedema in acute respiratory distress syndrome (ARDS). We developed the Radiographic Assessment of Lung Oedema (RALE) score to evaluate the extent and density of alveolar opacities on chest radiographs. After first comparing the RALE score to gravimetric assessment of pulmonary oedema in organ donors, we then evaluated the RALE score in patients with ARDS for its relationship to oxygenation and clinical outcomes.
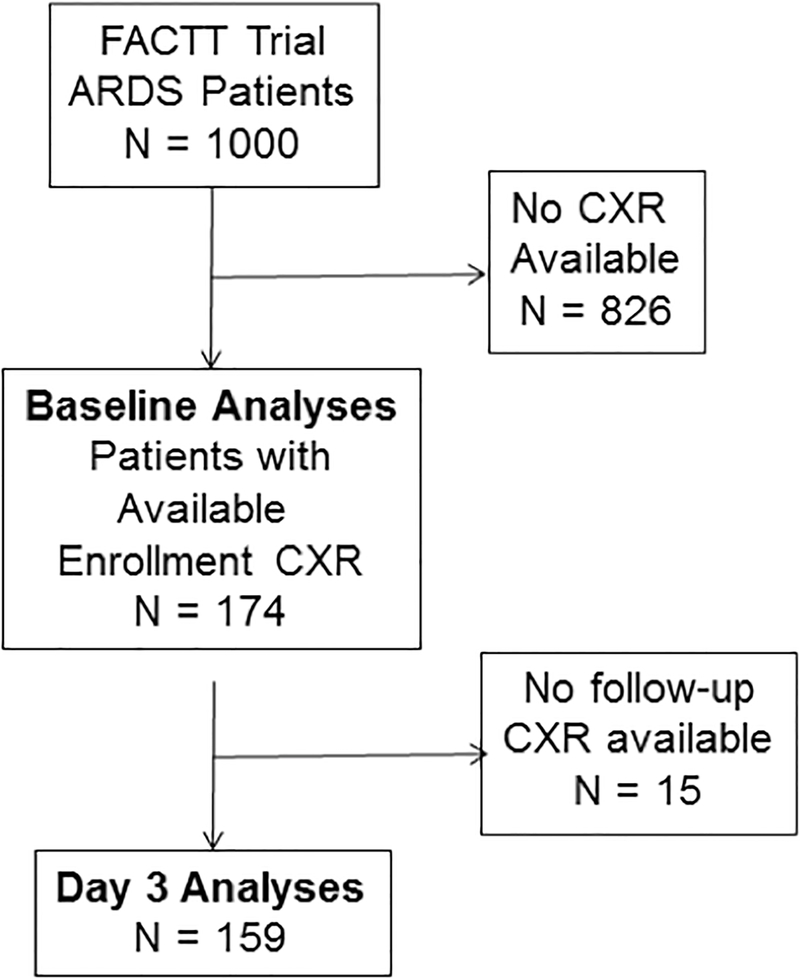
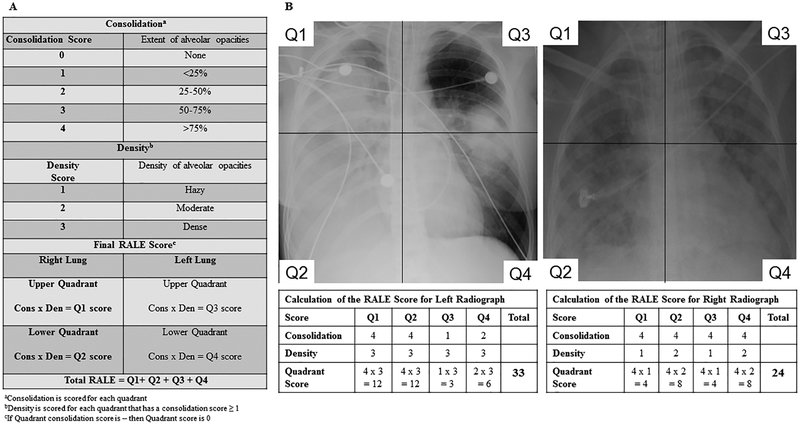
Methods: We compared radiographs with excised lung weights from 72 organ donors (derivation cohort) and radiographs with clinical data from 174 patients with ARDS in the ARDSNet Fluid and Catheter Treatment Trial (validation cohort). To calculate RALE, each radiographic quadrant was scored for extent of consolidation (0-4) and density of opacification (1-3). The product of the consolidation and density scores for each of the four quadrants was summed (maximum score=48).
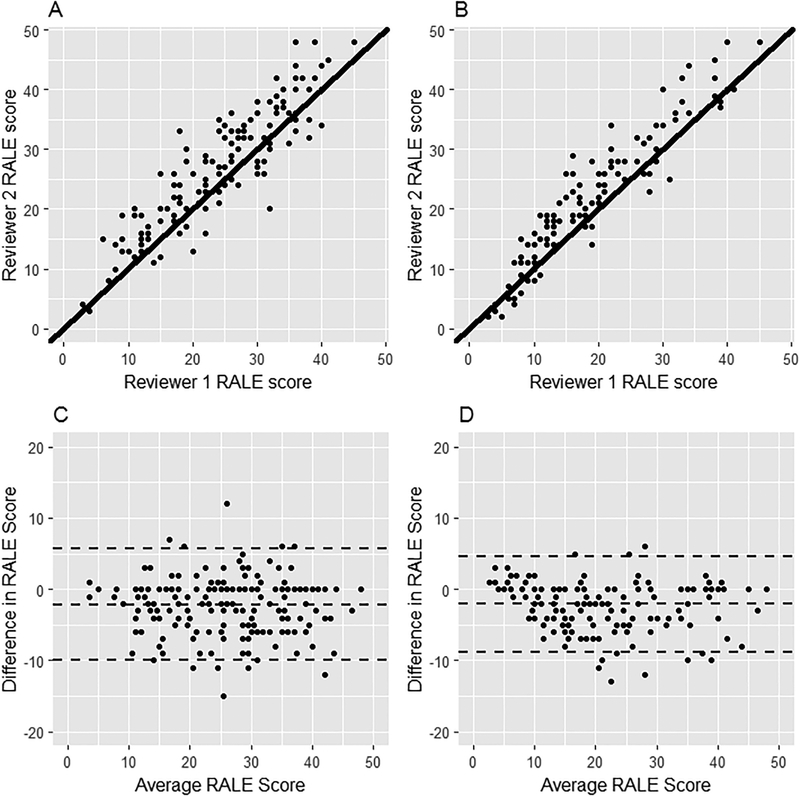
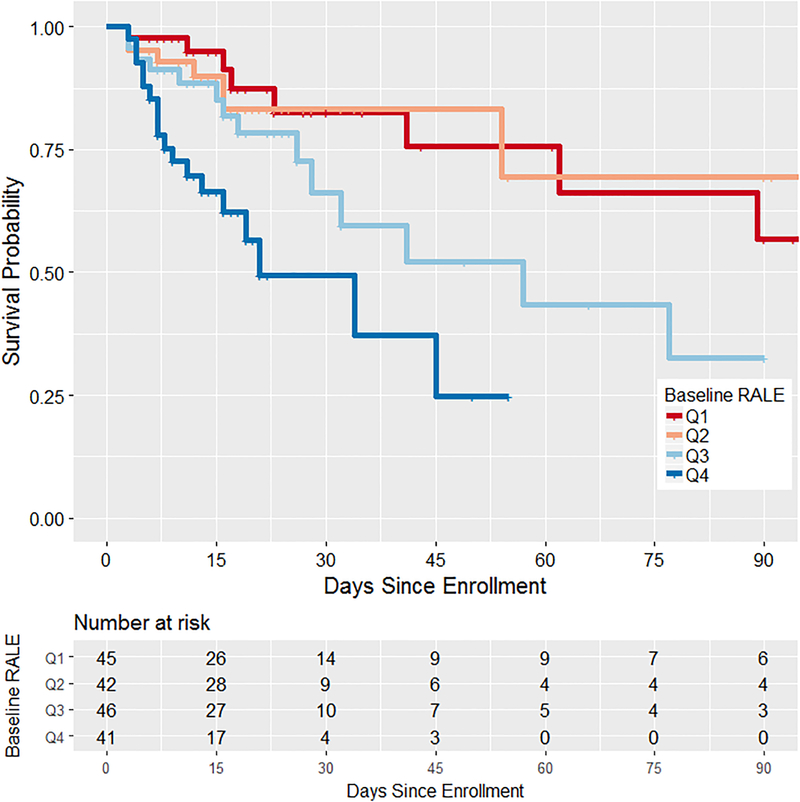
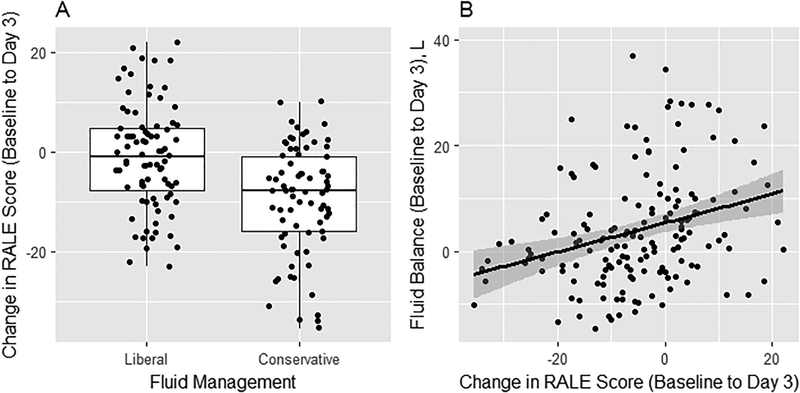
Results: Agreement between two independent reviewers for RALE score was excellent (intraclass correlation coefficient=0.93, 95% CI 0.91 to 0.95). In donors, pre-procurement RALE score correlated with height-adjusted total lung weight (ρ=0.59, p<0.001). In patients with ARDS, higher RALE scores were independently associated with lower PaO2/fractional inspired oxygen and worse survival. Conservative fluid management significantly decreased RALE score over 3 days compared with liberal fluid management.
Conclusions: The RALE score can be used to assess both the extent of pulmonary oedema and the severity of ARDS, by utilising information that is already obtained routinely, safely and inexpensively in every patient with ARDS. This novel non-invasive measure should be useful for assessing ARDS severity and monitoring response to therapy.
Keywords: ARDS; imaging/CT MRI etc; pulmonary oedema.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: JAB has received research funding from the National Institutes of Health and Global Blood Therapeutics. TWR has received consulting fees from Avisa Pharma and Cumberland Pharmaceuticals. CSC has received research funding from the National Institutes of Health, the Food and Drug Administration (FDA), the Department of Defense, Bayer and GlaxoSmithKline. She has received consulting fees from GlaxoSmithKline, Boehringer Ingelheim, Bayer, Prometic, CSL Behring and Roche/Genentech. MAM has received research grants from Amgen and GlaxoSmithKline and has a current research grant from Bayer Pharmaceuticals for ARDS studies. He has received consultation fees from CSL Behring, Boehinger Ingelheim, Cerus Therapeutics, Quark Pharmaceuticals, Thesan Pharmaceuticals and Bayer Pharmaceuticals. He was Chair of a DSMB for Asthma trials for Roche-Genentech (2013-2017). He also receives grant support for research and clinical trials from the NHLBI, FDA and the Department of Defense. LBW has received research funding from the National Institutes of Health, Boehringer Ingelheim and Global Blood Therapeutics and consultant fees from CSL Behring.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources