

Idiopathic intracranial hypertension: consensus guidelines on management
- PMID: 29903905
- PMCID: PMC6166610
- DOI: 10.1136/jnnp-2017-317440
Idiopathic intracranial hypertension: consensus guidelines on management
Abstract
The aim was to capture interdisciplinary expertise from a large group of clinicians, reflecting practice from across the UK and further, to inform subsequent development of a national consensus guidance for optimal management of idiopathic intracranial hypertension (IIH).
Methods: Between September 2015 and October 2017, a specialist interest group including neurology, neurosurgery, neuroradiology, ophthalmology, nursing, primary care doctors and patient representatives met. An initial UK survey of attitudes and practice in IIH was sent to a wide group of physicians and surgeons who investigate and manage IIH regularly. A comprehensive systematic literature review was performed to assemble the foundations of the statements. An international panel along with four national professional bodies, namely the Association of British Neurologists, British Association for the Study of Headache, the Society of British Neurological Surgeons and the Royal College of Ophthalmologists critically reviewed the statements.
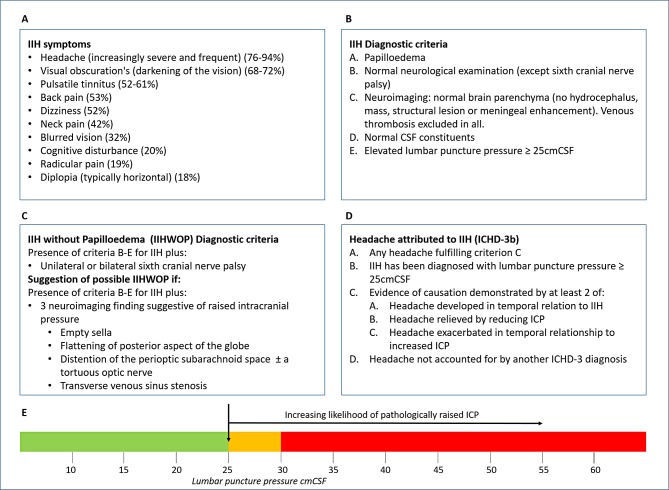
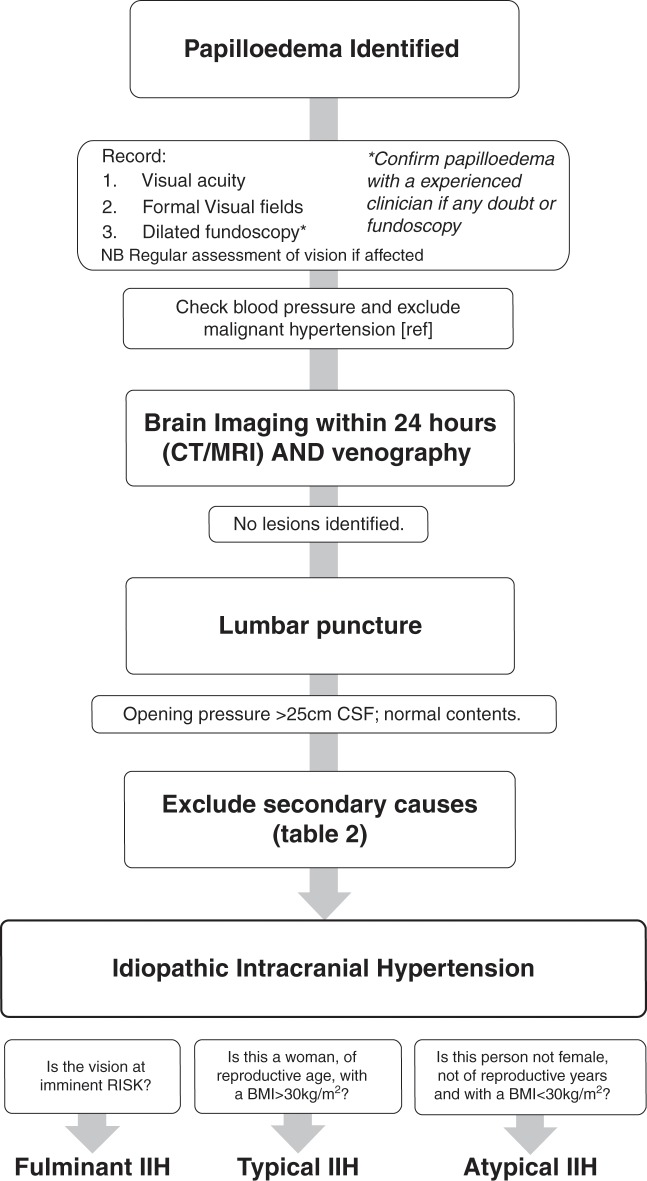
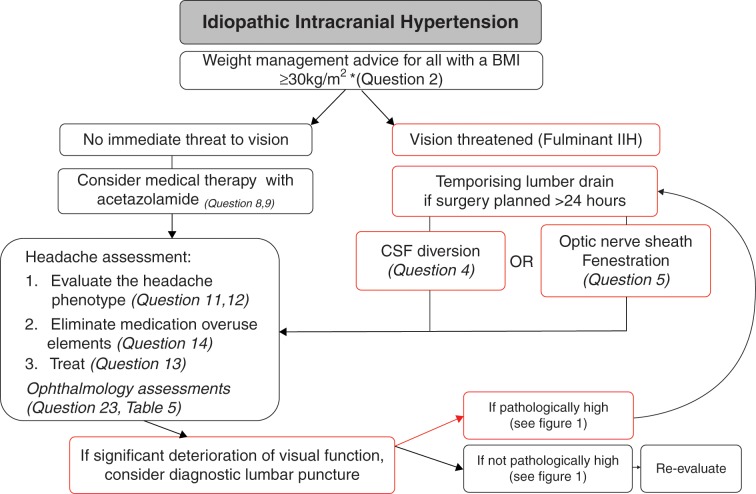
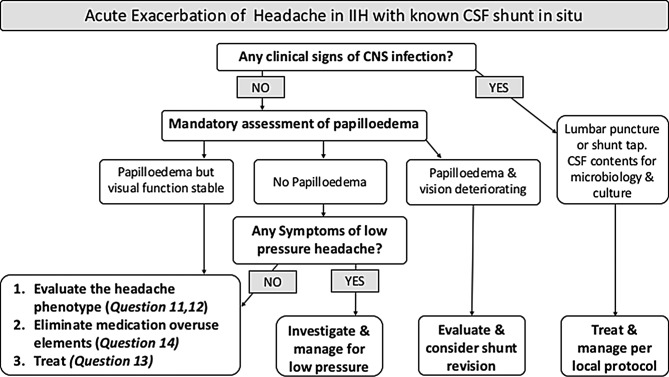
Results: Over 20 questions were constructed: one based on the diagnostic principles for optimal investigation of papilloedema and 21 for the management of IIH. Three main principles were identified: (1) to treat the underlying disease; (2) to protect the vision; and (3) to minimise the headache morbidity. Statements presented provide insight to uncertainties in IIH where research opportunities exist.
Conclusions: In collaboration with many different specialists, professions and patient representatives, we have developed guidance statements for the investigation and management of adult IIH.
Keywords: benign intracran hyp; clinical neurology; headache; neuroophthalmology; neurosurgery.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous