

Recent advances in field cancerization and management of multiple cutaneous squamous cell carcinomas
- PMID: 29904586
- PMCID: PMC5989149
- DOI: 10.12688/f1000research.12837.1
Recent advances in field cancerization and management of multiple cutaneous squamous cell carcinomas
Abstract
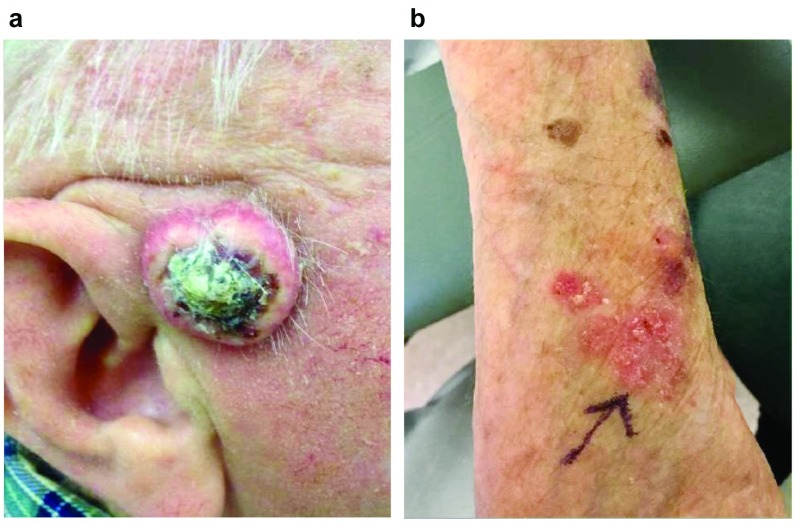
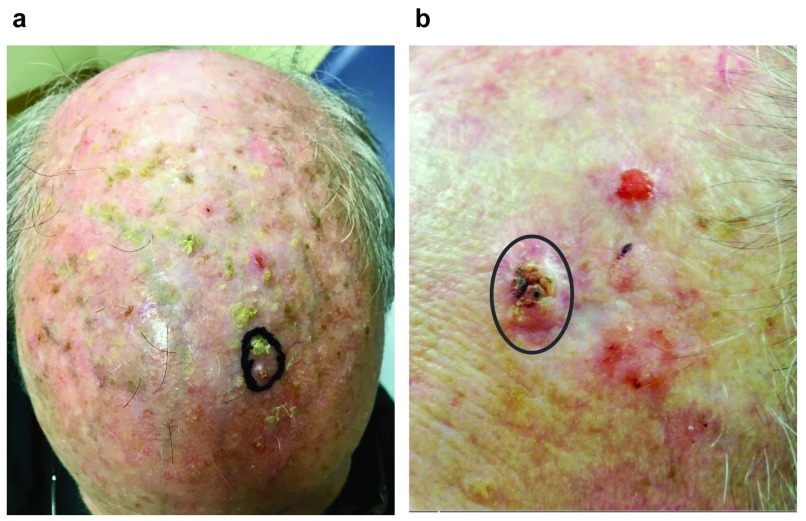
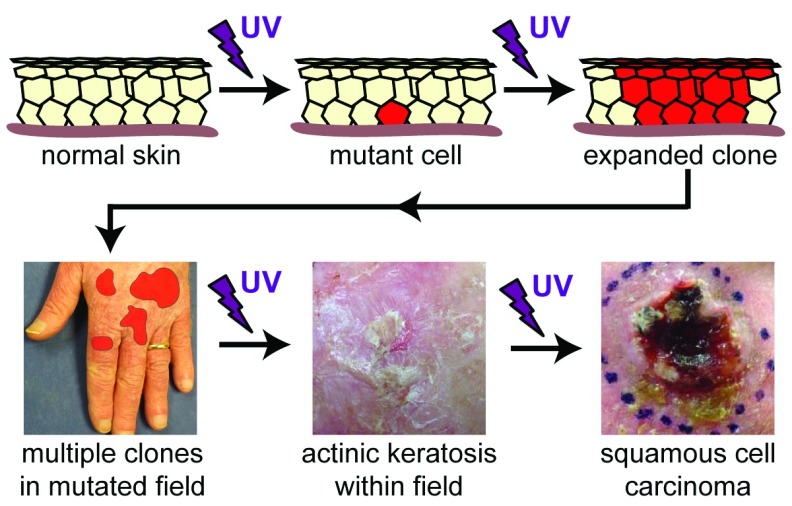
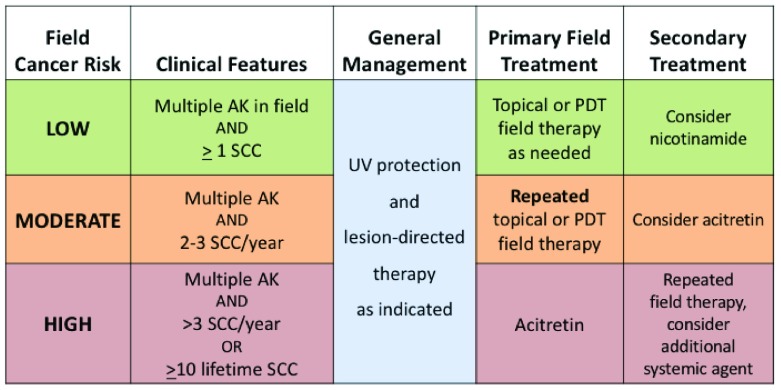
Cutaneous squamous cell carcinoma (SCC) is among the most common cancers in humans, and many patients with SCC will develop multiple tumors within their lifetime. The field cancerization concept, originally proposed over 60 years ago, hypothesized that multiple primary cancers may arise simultaneously and coexist with subclinical precursor lesions within a defined field. Genetic sequencing of SCC and precursor lesions has identified what may be the earliest clonal proliferations in SCC development and confirmed that field cancerization in the skin is mediated by ultraviolet radiation. For patients with multiple SCCs and severe actinic damage, treatment of precursor lesions within a cancerized field can decrease the risk of subsequent cancer development. Sunblock is an effective intervention for field cancerization, even in patients with established disease. There is now direct evidence that field therapy with topical 5-fluorouracil is effective in reducing the incidence of subsequent SCC, and there is indirect evidence suggesting that topical imiquimod, topical ingenol mebutate, and photodynamic therapy are similarly effective. There is limited direct evidence to show that systemic acitretin or nicotinamide can decrease incident SCC in patients with field cancerization. In this review, an approach to the management of patients with multiple SCCs and field cancerization is presented along with the rationale to support field-directed therapy.
Keywords: cutaneous squamous cell carcinoma; field cancerization; lesion-directed therapy.
Conflict of interest statement
No competing interests were disclosed.No competing interests were disclosed.No competing interests were disclosed.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials