

The value of 99mTc-MAA SPECT/CT for lung shunt estimation in 90Y radioembolization: a phantom and patient study
- PMID: 29904808
- PMCID: PMC6003896
- DOI: 10.1186/s13550-018-0402-8
The value of 99mTc-MAA SPECT/CT for lung shunt estimation in 90Y radioembolization: a phantom and patient study
Abstract
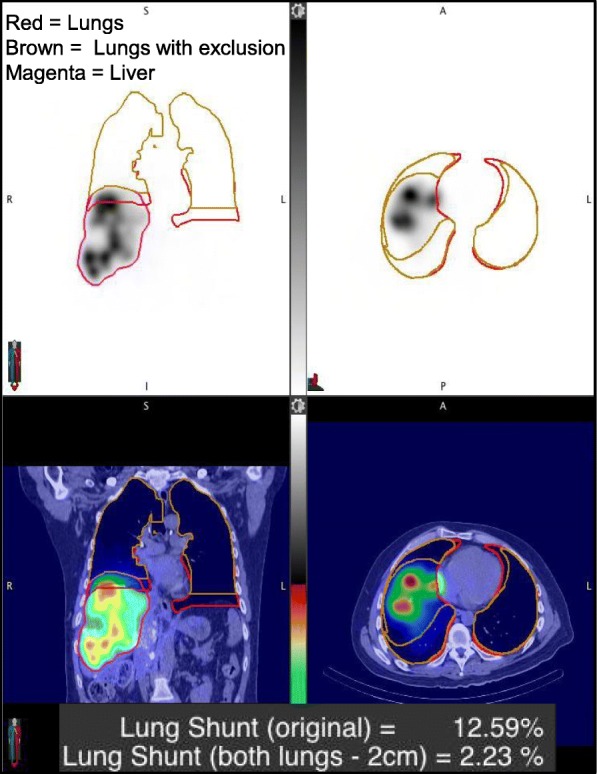
Background: A major toxicity concern in radioembolization therapy of hepatic malignancies is radiation-induced pneumonitis and sclerosis due to hepatopulmonary shunting of 90Y microspheres. Currently, 99mTc macroaggregated albumin (99mTc-MAA) imaging is used to estimate the lung shunt fraction (LSF) prior to treatment. The aim of this study was to evaluate the accuracy/precision of LSF estimated from 99mTc planar and SPECT/CT phantom imaging, and within this context, to compare the corresponding LSF and lung-absorbed dose values from 99mTc-MAA patient studies. Additionally, LSFs from pre- and post-therapy imaging were compared.
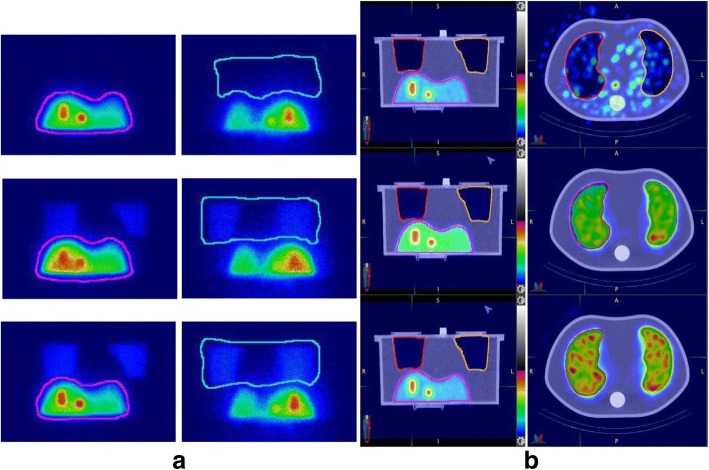
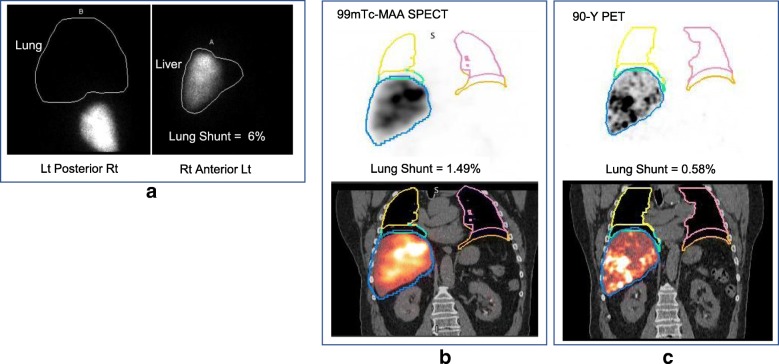
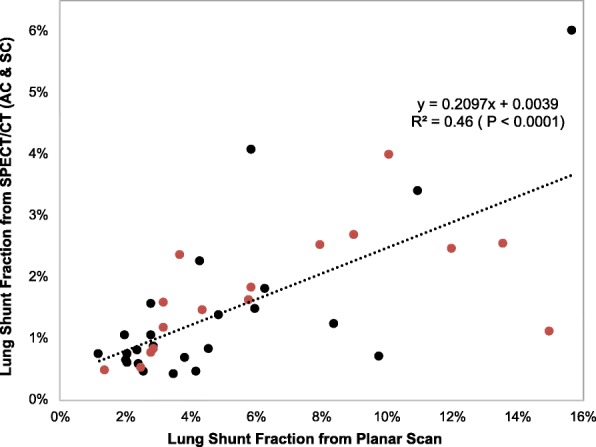
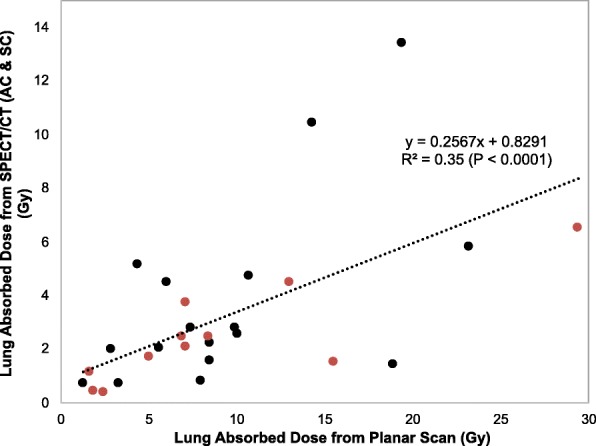
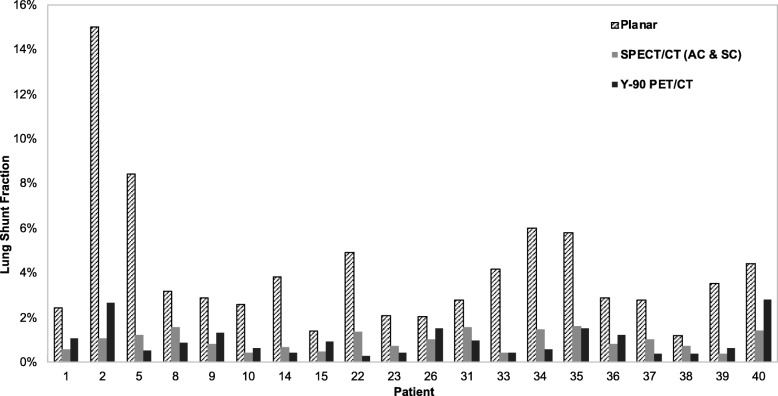
Results: A liver/lung torso phantom filled with 99mTc to achieve three lung shunt values was scanned by planar and SPECT/CT imaging with repeat acquisitions to assess accuracy and precision. To facilitate processing of patient data, a workflow that relies on SPECT and CT-based auto-contouring to define liver and lung volumes for the LSF calculation was implemented. Planar imaging-based LSF estimates for 40 patients, obtained from their medical records, were retrospectively compared with SPECT/CT imaging-based calculations with attenuation and scatter correction. Additionally, in a subset of 20 patients, the pre-therapy estimates were compared with 90Y PET/CT-based measurements. In the phantom study, improved accuracy in LSF estimation was achieved using SPECT/CT with attenuation and scatter correction (within 13% of the true value) compared with planar imaging (up to 44% overestimation). The results in patients showed a similar trend with planar imaging significantly overestimating LSF compared to SPECT/CT. There was no correlation between lung shunt estimates and the delay between 99mTc-MAA administration and scanning, but off-target extra hepatic uptake tended to be more likely in patients with a longer delay. The mean lung absorbed dose predictions for the 28 patients who underwent therapy was 9.3 Gy (range 1.3-29.4) for planar imaging and 3.2 Gy (range 0.4-13.4) for SPECT/CT. For the patients with post-therapy imaging, the mean LSF from 90Y PET/CT was 1.0%, (range 0.3-2.8). This value was not significantly different from the mean LSF estimate from 99mTc-MAA SPECT/CT (mean 1.0%, range 0.4-1.6; p = 0.968), but was significantly lower than the mean LSF estimate based on planar imaging (mean 4.1%, range 1.2-15.0; p = 0.0002).
Conclusions: The improved accuracy demonstrated by the phantom study, agreement with 90Y PET/CT in patient studies, and the practicality of using auto-contouring for liver/lung definition suggests that 99mTc-MAA SPECT/CT with scatter and attenuation corrections should be used for lung shunt estimation prior to radioembolization.
Keywords: 90Y PET/CT; 99mTc-MAA SPECT/CT; Lung shunt; Transarterial radioembolization (TARE).
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the University of Michigan Institutional Review Board, and all subjects signed an informed consent for 90Y PET/CT imaging and included consent to publish as part of an ongoing research study.
Consent for publication
All subjects signed an informed consent that included consent to publish data.
Competing interests
YKD is a consultant for MIM Software Inc., Beechwood, Ohio. The other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ho S, Lau WY, Leung TW, Chan M, et al. Clinical evaluation of the partition model for estimating radiation doses from yttrium-90 microspheres in the treatment of hepatic cancer. Eur J Nucl Med. 1997;24:293–298. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
