

Randomized, Double-Blind, Phase II Study of Temozolomide in Combination With Either Veliparib or Placebo in Patients With Relapsed-Sensitive or Refractory Small-Cell Lung Cancer
- PMID: 29906251
- PMCID: PMC6085179
- DOI: 10.1200/JCO.2018.77.7672
Randomized, Double-Blind, Phase II Study of Temozolomide in Combination With Either Veliparib or Placebo in Patients With Relapsed-Sensitive or Refractory Small-Cell Lung Cancer
Abstract
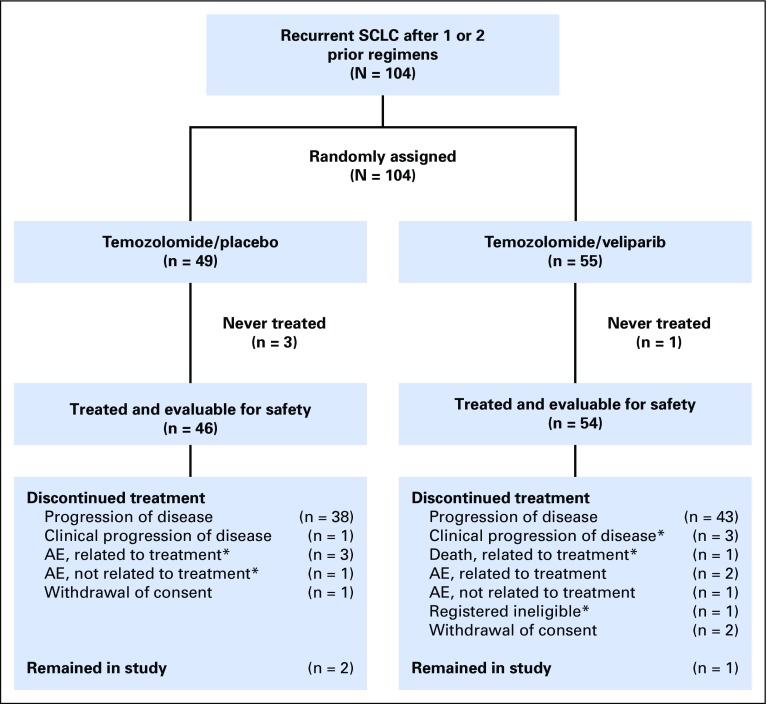
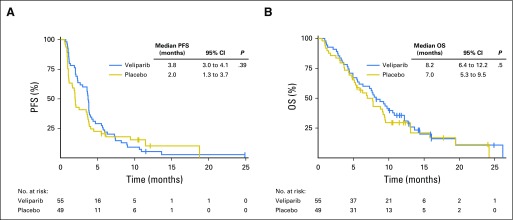
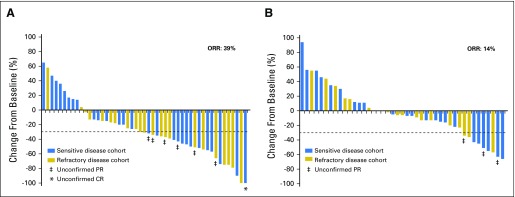
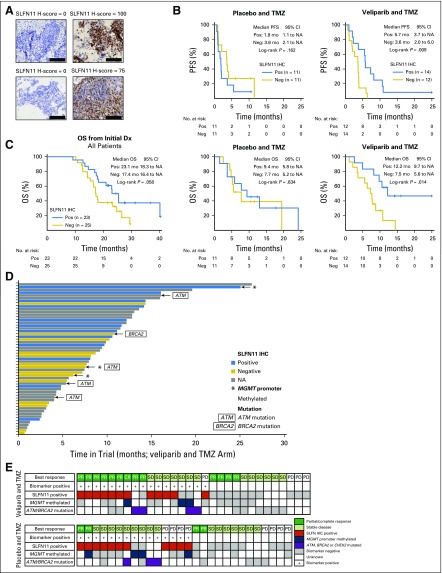
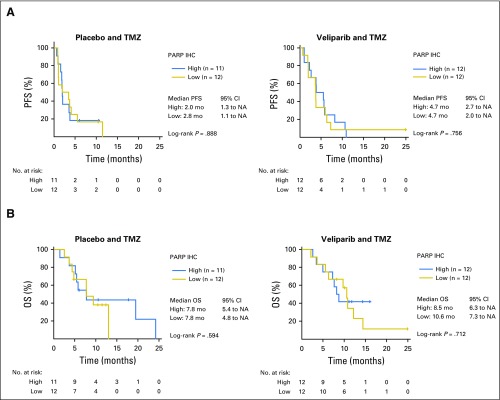
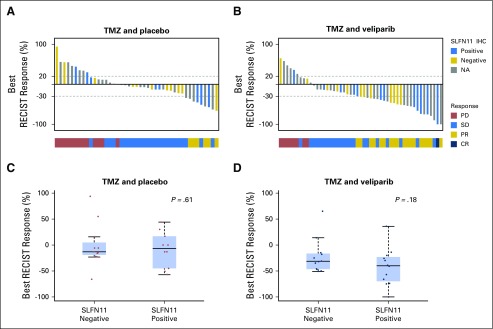
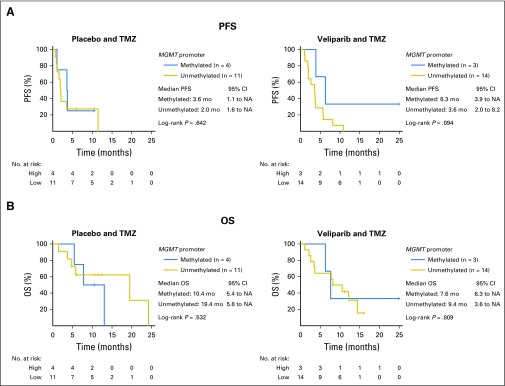
Purpose Both temozolomide (TMZ) and poly (ADP-ribose) polymerase (PARP) inhibitors are active in small-cell lung cancer (SCLC). This phase II, randomized, double-blind study evaluated whether addition of the PARP inhibitor veliparib to TMZ improves 4-month progression-free survival (PFS). Patients and Methods A total of 104 patients with recurrent SCLC were randomly assigned 1:1 to oral veliparib or placebo 40 mg twice daily, days 1 to 7, and oral TMZ 150 to 200 mg/m2/day, days 1 to 5, of a 28-day cycle until disease progression, unacceptable toxicity, or withdrawal of consent. Response was determined by imaging at weeks 4 and 8, and every 8 weeks thereafter. Improvement in PFS at 4 months was the primary end point. Secondary objectives included overall response rate (ORR), overall survival (OS), and safety and tolerability of veliparib with TMZ. Exploratory objectives included PARP-1 and SLFN11 immunohistochemical expression, MGMT promoter methylation, and circulating tumor cell quantification. Results No significant difference in 4-month PFS was noted between TMZ/veliparib (36%) and TMZ/placebo (27%; P = .19); median OS was also not improved significantly with TMZ/veliparib (8.2 months; 95% CI, 6.4 to 12.2 months; v 7.0 months; 95% CI, 5.3 to 9.5 months; P = .50). However, ORR was significantly higher in patients receiving TMZ/veliparib compared with TMZ/placebo (39% v 14%; P = .016). Grade 3/4 thrombocytopenia and neutropenia more commonly occurred with TMZ/veliparib: 50% versus 9% and 31% versus 7%, respectively. Significantly prolonged PFS (5.7 v 3.6 months; P = .009) and OS (12.2 v 7.5 months; P = .014) were observed in patients with SLFN11-positive tumors treated with TMZ/veliparib. Conclusion Four-month PFS and median OS did not differ between the two arms, whereas a significant improvement in ORR was observed with TMZ/veliparib. SLFN11 expression was associated with improved PFS and OS in patients receiving TMZ/veliparib, suggesting a promising biomarker of PARP-inhibitor sensitivity in SCLC.
Trial registration: ClinicalTrials.gov NCT01638546.
Figures
Comment in
-
SLFN11: a new synthetic lethal target?Nat Rev Clin Oncol. 2018 Sep;15(9):533. doi: 10.1038/s41571-018-0064-5. Nat Rev Clin Oncol. 2018. PMID: 29959392 No abstract available.
-
Is SLFN11 a Promising Predictive Biomarker of Poly (ADP-ribose) Polymerase Inhibitor Sensitivity in Small-Cell Lung Cancer? Not Yet!J Clin Oncol. 2019 Jan 20;37(3):259. doi: 10.1200/JCO.18.00993. Epub 2018 Nov 29. J Clin Oncol. 2019. PMID: 30496012 No abstract available.
-
Reply to F. Liang.J Clin Oncol. 2019 Jan 20;37(3):259. doi: 10.1200/JCO.18.01153. Epub 2018 Nov 29. J Clin Oncol. 2019. PMID: 30496013 No abstract available.
-
Sleep better on combination therapy: SLFN11 predicts response to veliparib and temozolomide in recurrent small cell lung cancer.Transl Lung Cancer Res. 2018 Dec;7(Suppl 4):S308-S311. doi: 10.21037/tlcr.2018.12.11. Transl Lung Cancer Res. 2018. PMID: 30705842 Free PMC article. No abstract available.
-
Temozolomide in combination with either veliparib or placebo in patients with relapsed-sensitive or refractory small-cell lung cancer.Transl Lung Cancer Res. 2018 Dec;7(Suppl 4):S329-S333. doi: 10.21037/tlcr.2018.12.02. Transl Lung Cancer Res. 2018. PMID: 30705847 Free PMC article. No abstract available.
-
Schlafen-11 (SLFN11): a step forward towards personalized medicine in small-cell lung cancer?Transl Lung Cancer Res. 2018 Dec;7(Suppl 4):S341-S345. doi: 10.21037/tlcr.2018.11.06. Transl Lung Cancer Res. 2018. PMID: 30705850 Free PMC article. No abstract available.
References
-
- von Pawel J, Schiller JH, Shepherd FA, et al. : Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J Clin Oncol 17:658-667, 1999 - PubMed
-
- O’Brien ME, Ciuleanu TE, Tsekov H, et al. : Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol 24:5441-5447, 2006 - PubMed
-
- Eckardt JR, von Pawel J, Pujol JL, et al. : Phase III study of oral compared with intravenous topotecan as second-line therapy in small-cell lung cancer. J Clin Oncol 25:2086-2092, 2007 - PubMed
-
- Eckardt J, Gralla R, Palmer MC, et al: Topotecan as second-line therapy in patients with small cell lung cancer: A phase II study. Ann Oncol 7:107, 1996 (abstr 513)
-
- Ardizzoni A, Hansen H, Dombernowsky P, et al. : Topotecan, a new active drug in the second-line treatment of small-cell lung cancer: A phase II study in patients with refractory and sensitive disease. The European Organization for Research and Treatment of Cancer Early Clinical Studies Group and New Drug Development Office, and the Lung Cancer Cooperative Group. J Clin Oncol 15:2090-2096, 1997 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
