

Microorganisms resistant to conventional antimicrobials in acute exacerbations of chronic obstructive pulmonary disease
- PMID: 29907113
- PMCID: PMC6003174
- DOI: 10.1186/s12931-018-0820-1
Microorganisms resistant to conventional antimicrobials in acute exacerbations of chronic obstructive pulmonary disease
Abstract
Background: Antimicrobial treatment for acute exacerbations of chronic obstructive pulmonary disease (AECOPD) remains controversial. In some cases AECOPD are caused by microorganisms that are resistant to treatments recommended by guidelines. Our aims were: 1) identify the risk factors associated with infection by microorganisms resistant to conventional treatment (MRCT), 2) Compare the clinical characteristics and outcomes of patients with AECOPD resulting from MRCT against those with AECOPD from other causes.
Methods: We prospective analysed a cohort of patients admitted with severe AECOPD (2009 to 2015) who were assigned to three groups: patients with MRCT (those patients with germs resistant to antibiotics recommended in guidelines), patients with microorganisms sensitive to conventional antimicrobial treatment (MSCT), and patients with negative microbiology results who had not previously received antibiotics. Multinomial logistic regression analyses were used to examine the associations between microbial aetiology groups and risk factors. The association between LOS and risk factors was also tested in simple and multiple analyses, and similar inclusion criteria were applied for the linear regression analysis.
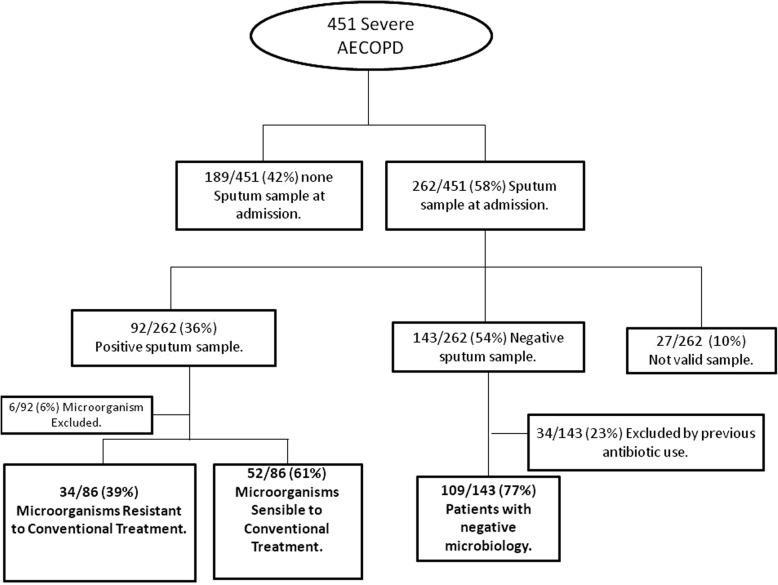
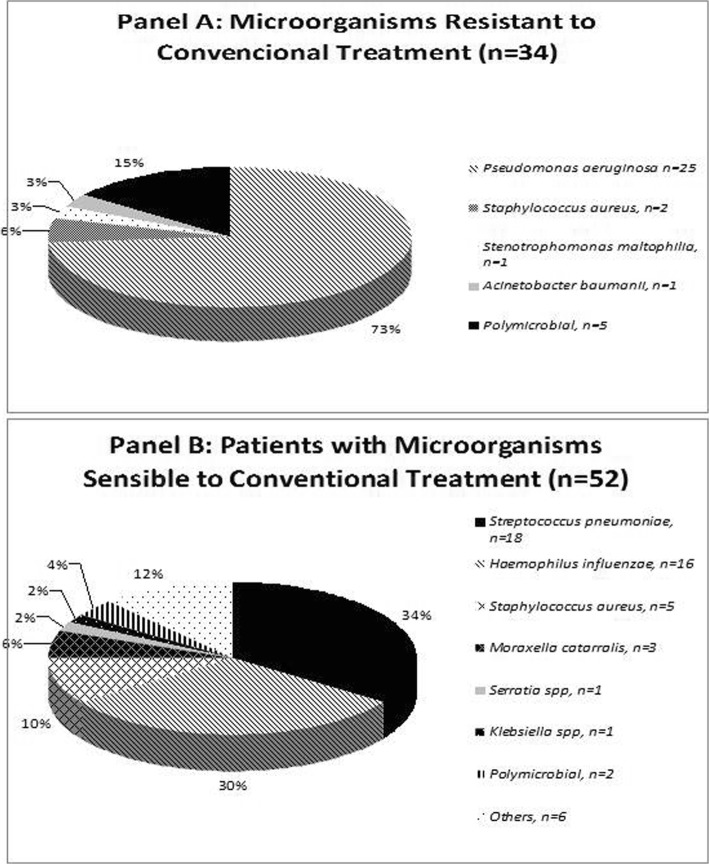
Results: Of the 451 patients admitted, 195 patients (43%) were included. Respiratory cultures were positive in 86(44%) and negative in 109(56%). MRCT were isolated in 34 cases (40%) and MSCT in 52 (60%). Patients with MRCT had more AECOPD in the previous year, received more antibiotic treatment in the previous three months, had more severe disease, higher dyspnoea and a positive respiratory culture in the previous year (mainly for Pseudomonas aeruginosa). The following conditions were independent factors for MRCT isolation: non-current smoker (odds ratio [OR] 4.19 [95% confidence interval [CI] 1.29-13.67], p = 0.017), ≥ 2 AECOPD or ≥ 1 admission for AECOPD in the previous year (OR 4.13 [95% CI 1.52-11.17], p = 0.005), C-reactive protein < 5 mg/dL; (OR 3.58 [95% CI 1.41-9.07], p = 0.007). Mortality rates were comparable at 30-days, one year and 3 years; however, patients in the MRCT group had longer hospital stays.
Conclusion: In conclusion, there are risk factors for resistant germs in AECOPD; however, the presence of these germs does not increase mortality. Patients with isolation of MRCT had longer length of stay.
Keywords: COPD; Exacerbation; Resistance to antimicrobials.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Hospital Research and Ethics Committee (CEIC 2008/4106) and the study was conducted in accordance with good clinical practice guidelines and the declaration of Helsinki. Written informed consent was obtained from all enrolled patients.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- From the Global Strategy for the Diagnosis, Management and Prevention of COPD Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017. Available http://www.goldcopd.org/. Accessed 1 Nov 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
