

Position of draining venous cannula in extracorporeal membrane oxygenation for respiratory and respiratory/circulatory support in adult patients
- PMID: 29907121
- PMCID: PMC6003129
- DOI: 10.1186/s13054-018-2083-0
Position of draining venous cannula in extracorporeal membrane oxygenation for respiratory and respiratory/circulatory support in adult patients
Abstract
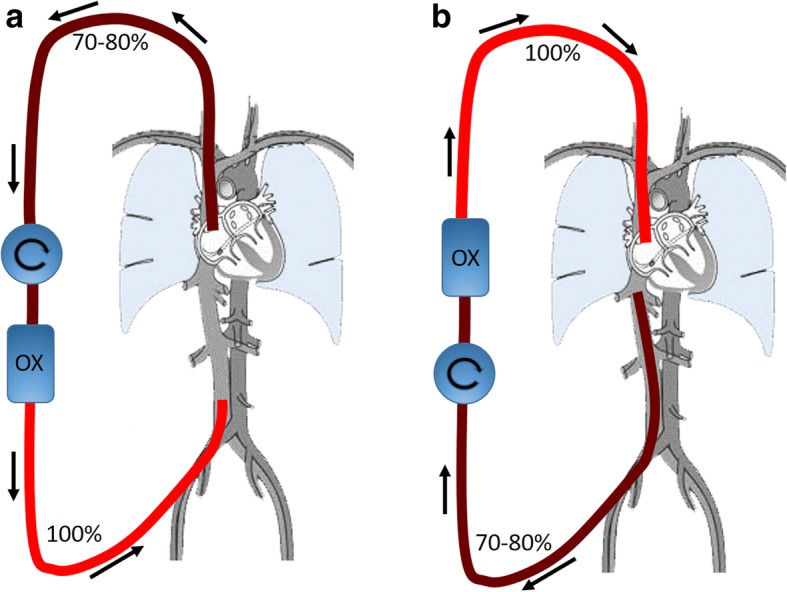
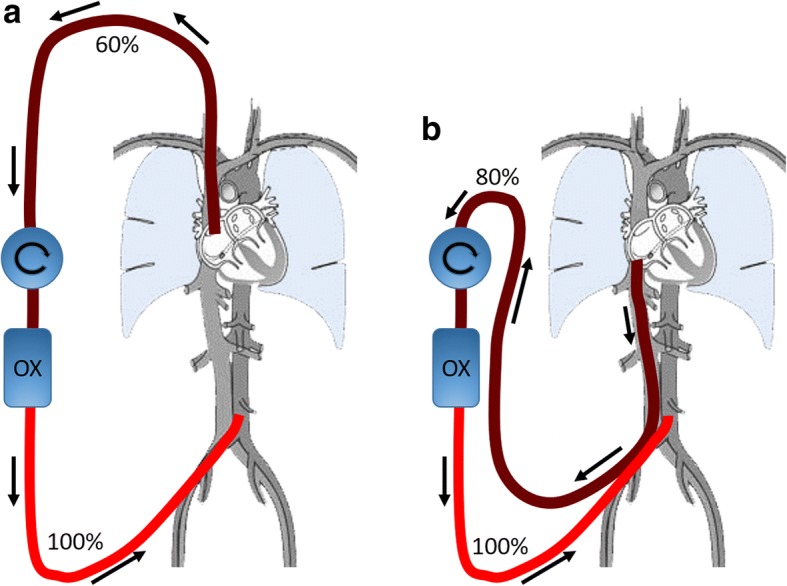
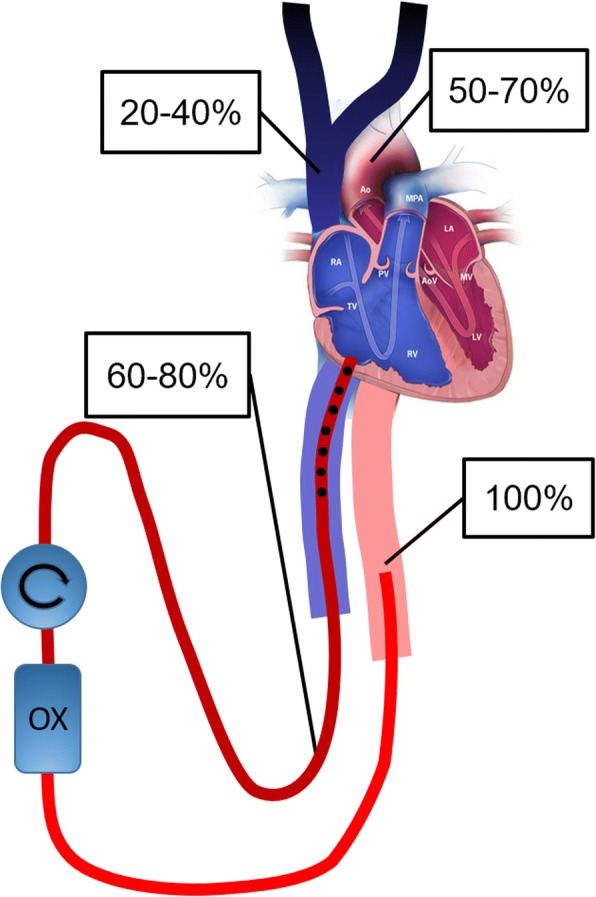
Extracorporeal membrane oxygenation (ECMO) is used in critically ill patients with severe pulmonary and/or cardiac failure. Blood is drained from the venous system and pumped through a membrane oxygenator where it is oxygenated. For pulmonary support, the blood is returned to the patient via a vein (veno-venous ECMO) and for pulmonary/circulatory support it is returned via an artery (veno-arterial ECMO).Veno-venous ECMO can be performed either with a single dual-lumen cannula or with two separate single-lumen cannulas. If the latter is chosen, flow direction can either be from the inferior caval vein (IVC) to the right atrium or the opposite. Earlier research has shown that drainage from the IVC yields less recirculation and therefore the IVC to right atrium route has become the standard in most centers for veno-venous ECMO with two cannulas. However, recent research has shown that recirculation can be minimized using a multistage draining cannula in the optimal position inserted via the right internal jugular vein and with blood return to the femoral vein. The clinical results with this route are excellent.In veno-arterial ECMO the most common site for blood infusion is the femoral artery. If venous blood is drained from the IVC, the patient is at risk of developing a dual circulation (Harlequin syndrome, North-South syndrome, differential oxygenation) meaning a poor oxygenation of the upper part of the body, while the lower part has excellent oxygenation. By instead draining from the superior caval vein (SVC) via a multistage cannula inserted in the right internal jugular vein this risk is neutralized.In conclusion, the authors argue that draining blood from the SVC and right atrium via a multistage cannula inserted in the right internal jugular vein is equal or better than IVC drainage both in veno-venous two cannula ECMO and in veno-arterial ECMO with blood return to the femoral artery.
Keywords: Differential hypoxemia; Draining cannula; Dual circulation; Flow direction; North-south syndrome; Recirculation; Veno-arterial ECMO; Veno-venous ECMO.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bartlett RH, Roloff DW, Cornell RG, Andrews AF, Dillon PW, Zwischenberger JB. Extracorporeal circulation in neonatal respiratory failure: a prospective randomized study. Pediatrics. 1985;76(4):479–487. - PubMed
-
- O'Rourke PP, Crone RK, Vacanti JP, Ware JH, Lillehei CW, Parad RB, Epstein MF. Extracorporeal membrane oxygenation and conventional medical therapy in neonates with persistent pulmonary hypertension of the newborn: a prospective randomized study. Pediatrics. 1989;84(6):957–963. - PubMed
-
- Peek GJ, Mugford M, Tiruvoipati R, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374(9698):1351–1363. doi: 10.1016/S0140-6736(09)61069-2. - DOI - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
