

Acute kidney injury is associated with a decrease in cortical renal perfusion during septic shock
- PMID: 29907130
- PMCID: PMC6002990
- DOI: 10.1186/s13054-018-2067-0
Acute kidney injury is associated with a decrease in cortical renal perfusion during septic shock
Abstract
Background: Renal perfusion status remains poorly studied at the bedside during septic shock. We sought to measure cortical renal perfusion in patients with septic shock during their first 3 days of care using renal contrast enhanced ultrasound (CEUS).
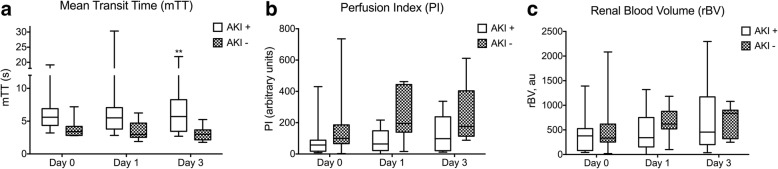
Methods: We prospectively included 20 ICU patients with septic shock and 10 control patients (CL) without septic shock admitted to a surgical ICU. Cortical renal perfusion was evaluated with CEUS during continuous infusion of Sonovue (Milan, Italy) within the first 24 h (day 0), between 24 and 48 h (day 1) and after 72 h (day 3) of care. Each measurement consisted of three destruction replenishment sequences that were recorded for delayed analysis with dedicated software (Vuebox). Renal perfusion was quantified by measuring the mean transit time (mTT) and the perfusion index (PI), which is the ratio of renal blood volume (rBV) to mTT.
Results: Cortical renal perfusion was decreased in septic shock as attested by a lower PI and a higher mTT in patients with septic shock than in patients of the CL group (p = 0.005 and p = 0.03). PI values had wider range in patients with septic shock (median (min-max) of 74 arbitrary units (a.u.) (3-736)) than in patients of the CL group 228 a.u. (67-440)). Renal perfusion improved over the first 3 days with a PI at day 3 higher than the PI at day 0 (74 (22-120) versus 160 (88-245) p = 0.02). mTT was significantly higher in patients with severe acute kidney injury (AKI) (n = 13) compared with patients with no AKI (n = 7) over time (p = 0.005). The PI was not different between patients with septic shock with severe AKI and those with no AKI (p = 0.29).
Conclusions: Although hemodynamic macrovascular parameters were restored, the cortical renal perfusion can be decreased, normal or even increased during septic shock. We observed an average decrease in cortical renal perfusion during septic shock compared to patients without septic shock. The decrease in cortical renal perfusion was associated with severe AKI occurrence. The use of renal CEUS to guide renal perfusion resuscitation needs further investigation.
Keywords: Acute kidney injury; Renal failure; Renal perfusion; Renal ultrasonography; Sepsis; Septic shock.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the comité d’Evaluation de l’Ethique des projets de Recherche Biomédicale (CEERB) du Groupe Hospitalier Universitaire (GHU) Nord (Institutional Review Board (IRB) of Paris North Hospitals, Paris 7 University, AP-HP) with the number 11-065. The institutional Review Board waived the need for informed consent.
Consent for publication
The manuscript does not contain any individual person’s data in any form.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Comment in
-
Is cortical perfusion a reliable marker for predicting septic acute kidney injury?Crit Care. 2019 Mar 22;23(1):94. doi: 10.1186/s13054-019-2386-9. Crit Care. 2019. PMID: 30902102 Free PMC article. No abstract available.
References
-
- Venot M, Weis L, Clec'h C, Allaouchiche B, Goldgran-Toledano D, Garrouste-Orgeas M, Adrie C, Timsit JF, Azoulay E, et al. Acute kidney injury in severe sepsis and septic shock in patients with and without diabetes mellitus: a multicenter study. PLoS One. 2015;10:e0127411. doi: 10.1371/journal.pone.0127411. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
