

Validation of a Natural Language Processing Algorithm for Detecting Infectious Disease Symptoms in Primary Care Electronic Medical Records in Singapore
- PMID: 29907560
- PMCID: PMC6026305
- DOI: 10.2196/medinform.8204
Validation of a Natural Language Processing Algorithm for Detecting Infectious Disease Symptoms in Primary Care Electronic Medical Records in Singapore
Abstract
Background: Free-text clinical records provide a source of information that complements traditional disease surveillance. To electronically harness these records, they need to be transformed into codified fields by natural language processing algorithms.
Objective: The aim of this study was to develop, train, and validate Clinical History Extractor for Syndromic Surveillance (CHESS), an natural language processing algorithm to extract clinical information from free-text primary care records.
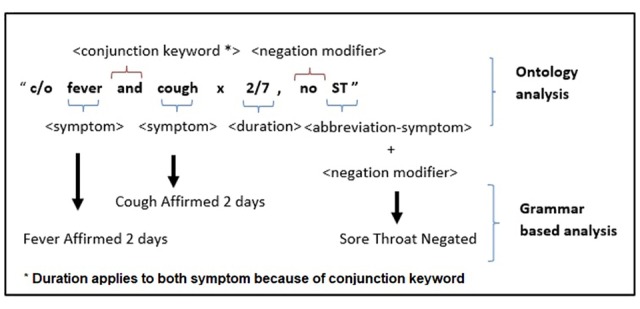
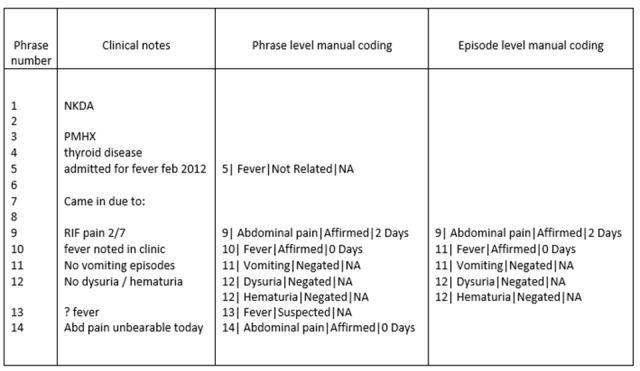
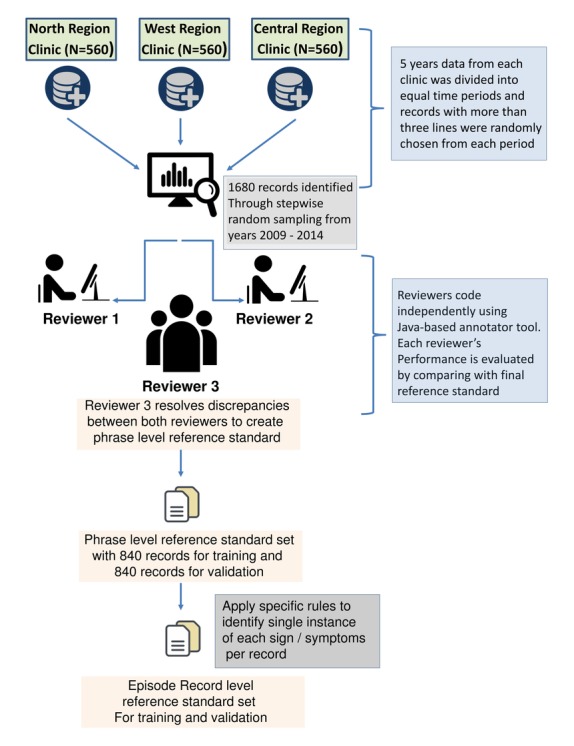
Methods: CHESS is a keyword-based natural language processing algorithm to extract 48 signs and symptoms suggesting respiratory infections, gastrointestinal infections, constitutional, as well as other signs and symptoms potentially associated with infectious diseases. The algorithm also captured the assertion status (affirmed, negated, or suspected) and symptom duration. Electronic medical records from the National Healthcare Group Polyclinics, a major public sector primary care provider in Singapore, were randomly extracted and manually reviewed by 2 human reviewers, with a third reviewer as the adjudicator. The algorithm was evaluated based on 1680 notes against the human-coded result as the reference standard, with half of the data used for training and the other half for validation.
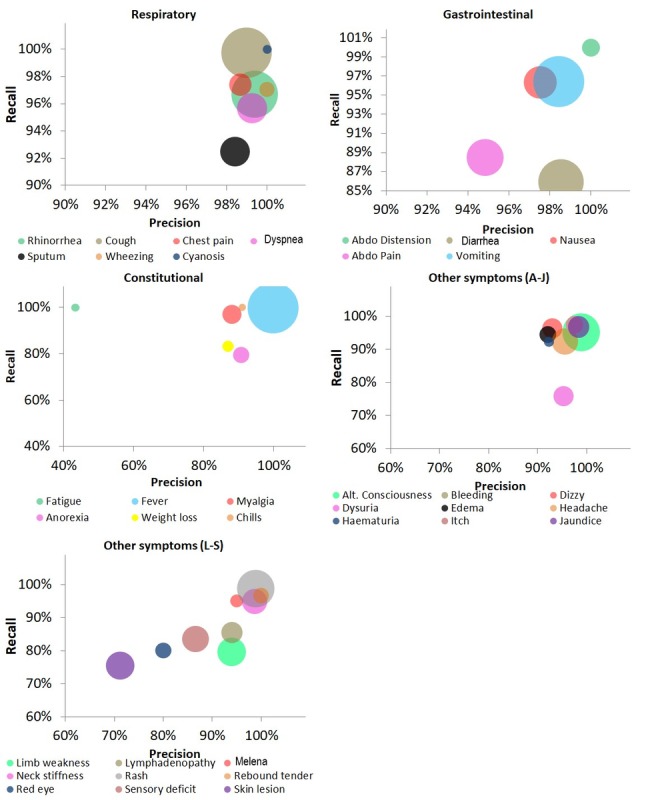
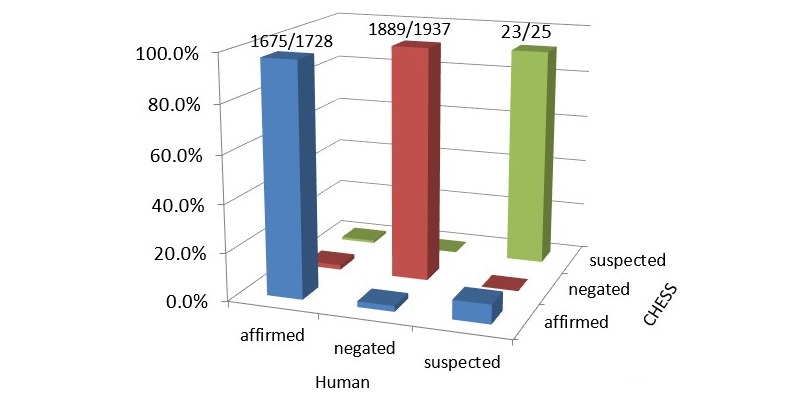
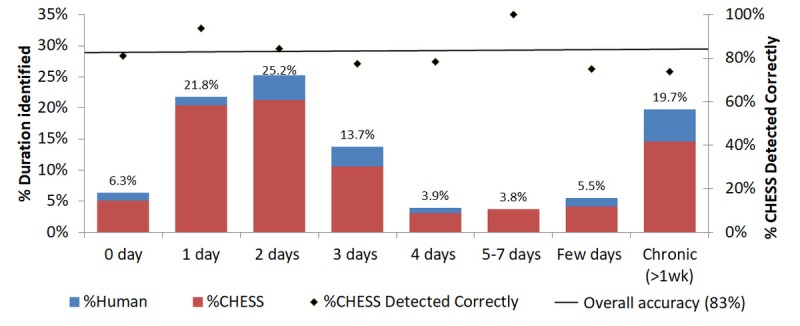
Results: The symptoms most commonly present within the 1680 clinical records at the episode level were those typically present in respiratory infections such as cough (744/7703, 9.66%), sore throat (591/7703, 7.67%), rhinorrhea (552/7703, 7.17%), and fever (928/7703, 12.04%). At the episode level, CHESS had an overall performance of 96.7% precision and 97.6% recall on the training dataset and 96.0% precision and 93.1% recall on the validation dataset. Symptoms suggesting respiratory and gastrointestinal infections were all detected with more than 90% precision and recall. CHESS correctly assigned the assertion status in 97.3%, 97.9%, and 89.8% of affirmed, negated, and suspected signs and symptoms, respectively (97.6% overall accuracy). Symptom episode duration was correctly identified in 81.2% of records with known duration status.
Conclusions: We have developed an natural language processing algorithm dubbed CHESS that achieves good performance in extracting signs and symptoms from primary care free-text clinical records. In addition to the presence of symptoms, our algorithm can also accurately distinguish affirmed, negated, and suspected assertion statuses and extract symptom durations.
Keywords: communicable diseases; electronic health records; epidemiology; natural language processing; surveillance; syndromic surveillance.
©Antony Hardjojo, Arunan Gunachandran, Long Pang, Mohammed Ridzwan Bin Abdullah, Win Wah, Joash Wen Chen Chong, Ee Hui Goh, Sok Huang Teo, Gilbert Lim, Mong Li Lee, Wynne Hsu, Vernon Lee, Mark I-Cheng Chen, Franco Wong, Jonathan Siung King Phang. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 11.06.2018.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Hope K, Durrheim DN, d'Espaignet ET, Dalton C. Syndromic surveillance: is it a useful tool for local outbreak detection? J Epidemiol Community Health. 2006 May;60(5):374–5. http://europepmc.org/abstract/MED/16680907 - PMC - PubMed
-
- Ministry of Health, Singapore 2018. [2018-02-05]. Communicable Diseases Surveillance in Singapore 2016 https://www.moh.gov.sg/content/moh_web/home/Publications/Reports/2017/co... .
-
- Levin JE, Raman S. Early detection of rotavirus gastrointestinal illness outbreaks by multiple data sources and detection algorithms at a pediatric health system. AMIA Annu Symp Proc. 2005:445–9. http://europepmc.org/abstract/MED/16779079 56946 - PMC - PubMed
-
- Buehler JW, Hopkins RS, Overhage JM, Sosin DM, Tong V, CDC Working Group Framework for evaluating public health surveillance systems for early detection of outbreaks: recommendations from the CDC Working Group. MMWR Recomm Rep. 2004 May 7;53(RR-5):1–11. http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5305a1.htm rr5305a1 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
