

Diagnostic yield and accuracy of coronary CT angiography after abnormal nuclear myocardial perfusion imaging
- PMID: 29907855
- PMCID: PMC6003932
- DOI: 10.1038/s41598-018-27347-8
Diagnostic yield and accuracy of coronary CT angiography after abnormal nuclear myocardial perfusion imaging
Abstract
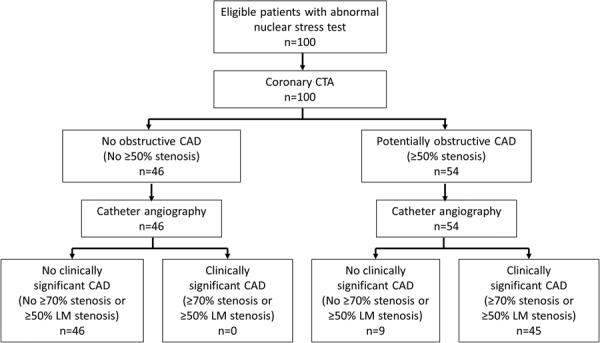
We aimed to determine the diagnostic yield and accuracy of coronary CT angiography (CCTA) in patients referred for invasive coronary angiography (ICA) based on clinical concern for coronary artery disease (CAD) and an abnormal nuclear stress myocardial perfusion imaging (MPI) study. We enrolled 100 patients (84 male, mean age 59.6 ± 8.9 years) with an abnormal MPI study and subsequent referral for ICA. Each patient underwent CCTA prior to ICA. We analyzed the prevalence of potentially obstructive CAD (≥50% stenosis) on CCTA and calculated the diagnostic accuracy of ≥50% stenosis on CCTA for the detection of clinically significant CAD on ICA (defined as any ≥70% stenosis or ≥50% left main stenosis). On CCTA, 54 patients had at least one ≥50% stenosis. With ICA, 45 patients demonstrated clinically significant CAD. A positive CCTA had 100% sensitivity and 84% specificity with a 100% negative predictive value and 83% positive predictive value for clinically significant CAD on a per patient basis in MPI positive symptomatic patients. In conclusion, almost half (48%) of patients with suspected CAD and an abnormal MPI study demonstrate no obstructive CAD on CCTA.
Conflict of interest statement
This study was supported by a research grant provided by GE Healthcare (Wauwatosa/WI/United States). UJS is a consultant for and/or receives institutional research support from Astellas, Bayer, Bracco, GE, Guerbet, HeartFlow, and Siemens Healthineers. FGM has received institutional research support from Siemens, unrelated to this investigation. The other authors declare that they have no competing interests.
Figures
References
-
- Knuuti, J. et al. Risks and benefits of cardiac imaging: an analysis of risks related to imaging for coronary artery disease. Eur Heart J (2013). - PubMed
-
- Meijboom WB, et al. Comprehensive assessment of coronary artery stenoses: computed tomography coronary angiography versus conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina. J Am Coll Cardiol. 2008;52:636–643. doi: 10.1016/j.jacc.2008.05.024. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
