

An Automated Multiparametric MRI Quantitative Imaging Prostate Habitat Risk Scoring System for Defining External Beam Radiation Therapy Boost Volumes
- PMID: 29908220
- PMCID: PMC6245650
- DOI: 10.1016/j.ijrobp.2018.06.003
An Automated Multiparametric MRI Quantitative Imaging Prostate Habitat Risk Scoring System for Defining External Beam Radiation Therapy Boost Volumes
Abstract
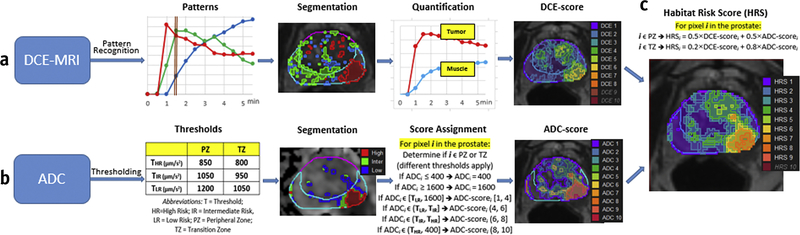
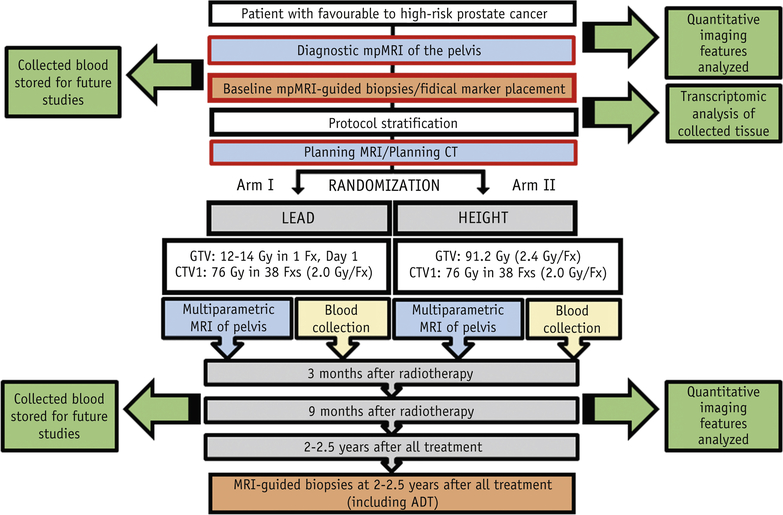
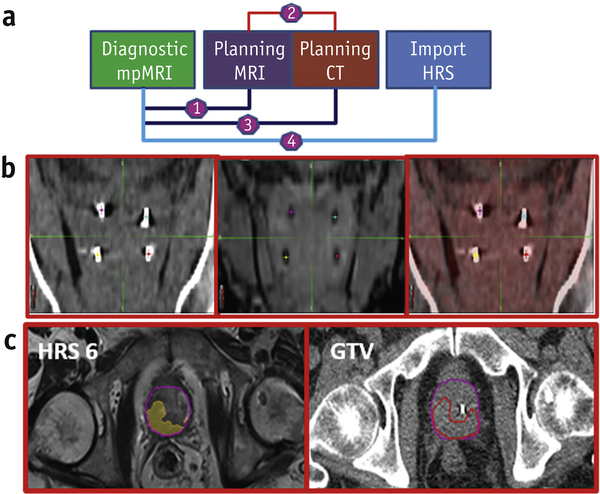
Purpose: To develop a prostate tumor habitat risk scoring (HRS) system based on multiparametric magnetic resonance imaging (mpMRI) referenced to prostatectomy Gleason score (GS) for automatic delineation of gross tumor volumes. A workflow for integration of HRS into radiation therapy boost volume dose escalation was developed in the framework of a phase 2 randomized clinical trial (BLaStM).
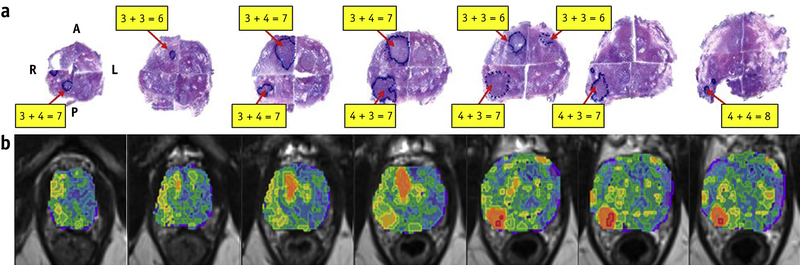
Methods and materials: An automated quantitative mpMRI-based 10-point pixel-by-pixel method was optimized to prostatectomy GSs and volumes using referenced dynamic contrast-enhanced and apparent diffusion coefficient sequences. The HRS contours were migrated to the planning computed tomography scan for boost volume generation.
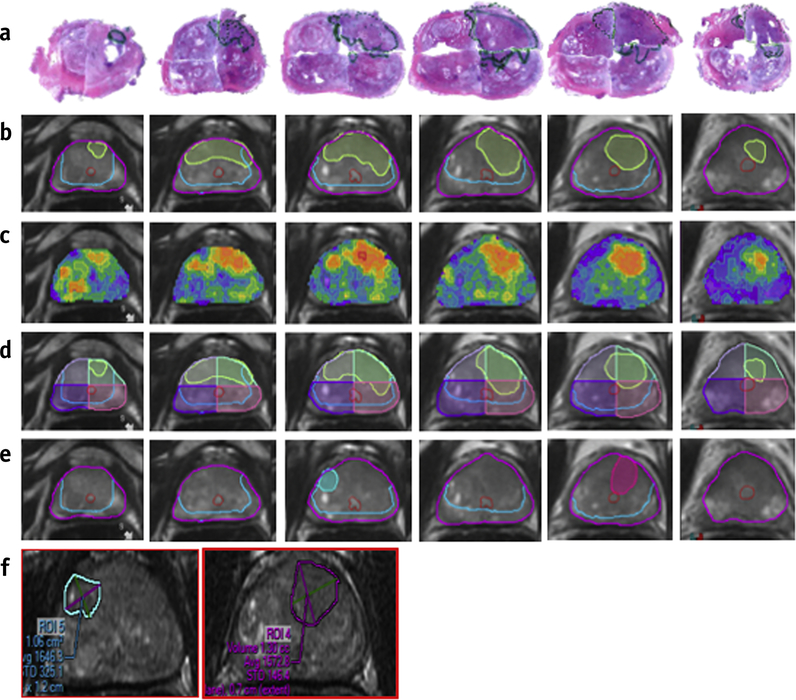
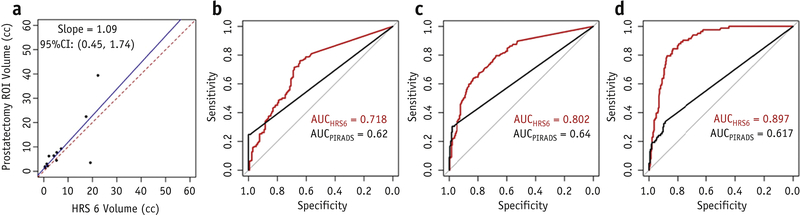
Results: There were 51 regions of interest in 12 patients who underwent radical prostatectomy (26 with GS ≥7 and 25 with GS 6). The resultant heat maps showed inter- and intratumoral heterogeneity. The HRS6 level was significantly associated with radical prostatectomy regions of interest (slope 1.09, r = 0.767; P < .0001). For predicting the likelihood of cancer, GS ≥7 and GS ≥8 HRS6 area under the curve was 0.718, 0.802, and 0.897, respectively. HRS was superior to the Prostate Imaging, Reporting and Diagnosis System 4/5 classification, wherein the area under the curve was 0.62, 0.64, and 0.617, respectively (difference with HR6, P < .0001). HRS maps were created for the first 37 assessable patients on the BLaStM trial. There were an average of 1.38 habitat boost volumes per patient at a total boost volume average of 3.6 cm3.
Conclusions: An automated quantitative mpMRI-based method was developed to objectively guide dose escalation to high-risk habitat volumes based on prostatectomy GS.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Morris WJ, Tyldesley S, Rodda S, et al. Androgen Suppression Combined with Elective Nodal and Dose Escalated Radiation Therapy (the ASCENDE-RT Trial): An Analysis of Survival Endpoints for a Randomized Trial Comparing a Low-Dose-Rate Brachytherapy Boost to a Dose-Escalated External Beam Boost for High- and Intermediate-risk Prostate Cancer. Int J Radiat Oncol Biol Phys. 2017;98(2):275–85. - PubMed
-
- Bauman G, Haider M, Van der Heide UA, Menard C. Boosting imaging defined dominant prostatic tumors: a systematic review. Radiother Oncol. 2013;107(3):274–81. - PubMed
-
- von Eyben FE, Kiljunen T, Kangasmaki A, et al. Radiotherapy Boost for the Dominant Intraprostatic Cancer Lesion-A Systematic Review and Meta-Analysis. Clin Genitourin Cancer. 2016;14(3):189–97. - PubMed
-
- Isebaert S, Van den Bergh L, Haustermans K, et al. Multiparametric MRI for prostate cancer localization in correlation to whole-mount histopathology. J Magn Reson Imaging. 2013;37(6):1392–401. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
