

Prevalence and Long-Term Survival After Coronary Artery Bypass Grafting in Women and Men With Heart Failure and Preserved Versus Reduced Ejection Fraction
- PMID: 29909401
- PMCID: PMC6220539
- DOI: 10.1161/JAHA.118.008902
Prevalence and Long-Term Survival After Coronary Artery Bypass Grafting in Women and Men With Heart Failure and Preserved Versus Reduced Ejection Fraction
Abstract
Background: Heart failure (HF) with reduced ejection fraction (rEF) is a widely regarded prognosticator after coronary artery bypass grafting. HF with preserved ejection fraction (pEF) accounts for up to half of all HF cases and is associated with considerable morbidity and mortality in hospitalized cohorts. However, HFpEF outcomes have not been elucidated in cardiac surgical patients. We investigated the prevalence and outcomes of HFpEF and HFrEF in women and men following coronary artery bypass grafting.
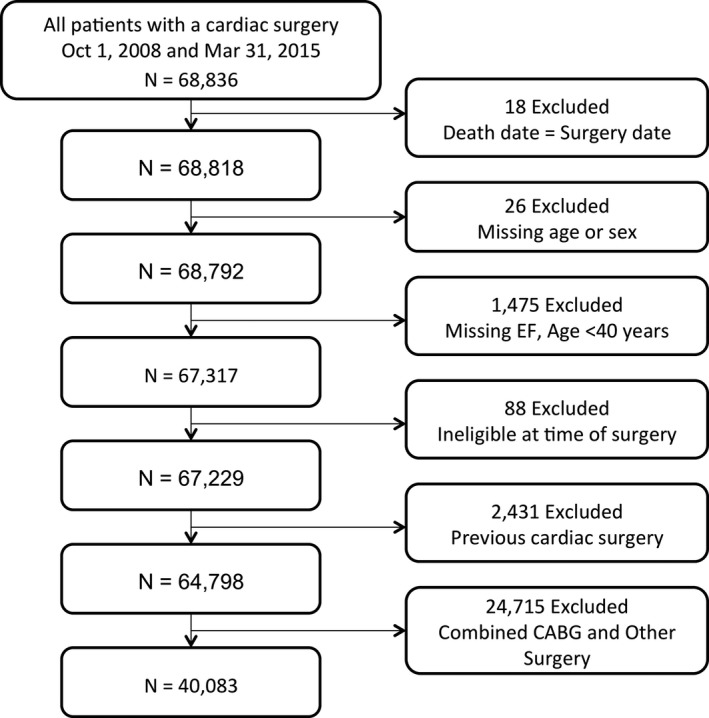
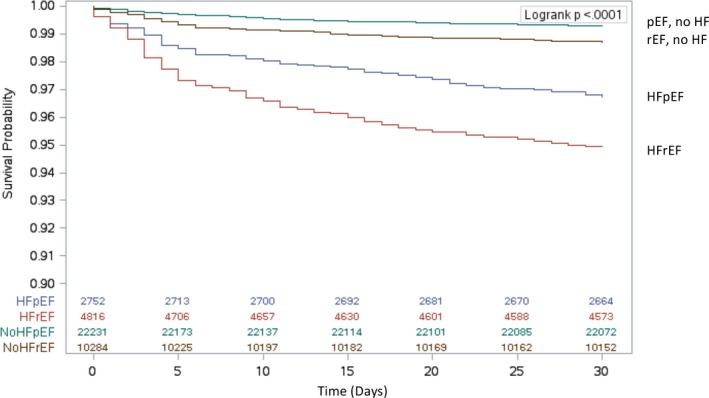
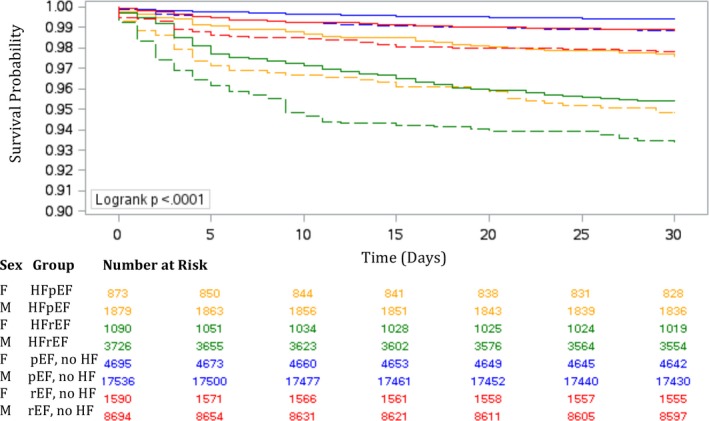
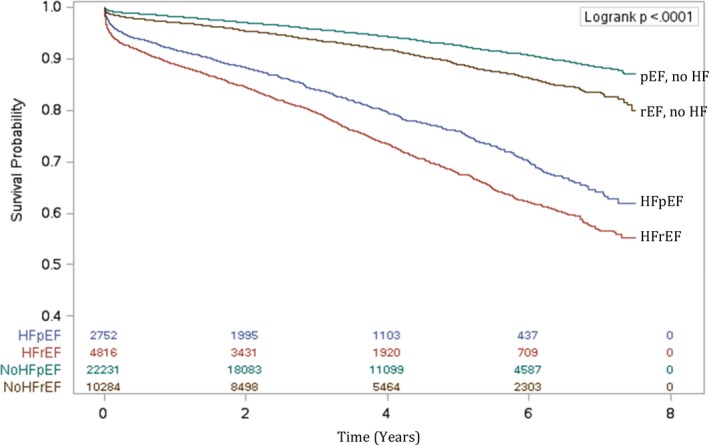
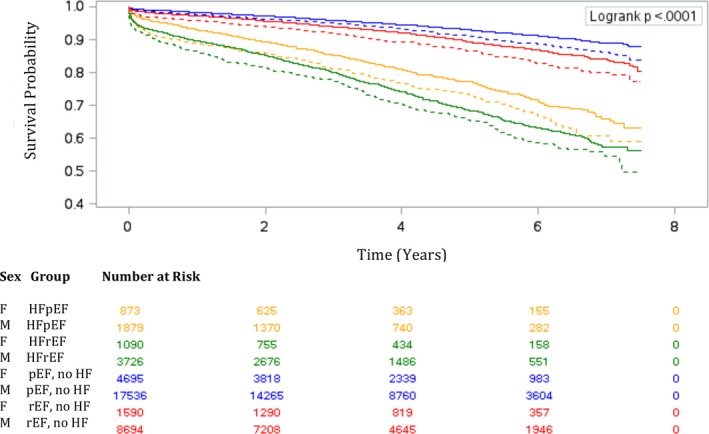
Methods and results: We conducted a retrospective cohort study in Ontario, Canada, between October 1, 2008, and March 31, 2015, using Cardiac Care Network and Canadian Institute of Health Information data. HF is captured through a validated population-based database of all Ontarians with physician-diagnosed HF. We defined pEF as ejection fraction ≥50% and rEF as ejection fraction <50%. The primary outcome was all-cause mortality. Analyses were stratified by sex. Mortality rates were calculated using Kaplan-Meier method. The relative hazard of death was assessed using multivariable Cox proportional hazard models. Of 40 083 patients (20.6% women), 55.5% had pEF without HF, 25.7% had rEF without HF, 6.9% had HFpEF, and 12.0% had HFrEF. Age-standardized HFpEF mortality rates at 4±2 years of follow-up were similar in women and men. HFrEF standardized HFpEF mortality rates were higher in women than men.
Conclusions: We found a higher prevalence and poorer prognosis of HFpEF in women. A history of HF was a more important prognosticator than ejection fraction. Preoperative screening and extended postoperative follow-up should be focused on women and men with HF rather than on rEF alone.
Keywords: coronary artery bypass graft surgery; ejection fraction; heart failure; heart failure with preserved ejection fraction; heart failure with reduced ejection fraction; mortality; prognosis; sex.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Wrobel K, Stevens SR, Jones RH, Selzman CH, Lamy A, Beaver TM, Djokovic LT, Wang N, Velazquez EJ, Sopko G, Kron IL, DiMaio JM, Michler RE, Lee KL, Yii M, Leng CY, Zembala M, Rouleau JL, Daly RC, Al‐Khalidi HR. Influence of baseline characteristics, operative conduct, and postoperative course on 30‐day outcomes of coronary artery bypass grafting among patients with left ventricular dysfunction: results from the surgical treatment for ischemic heart failure (STICH) trial. Circulation. 2015;132:720–730. - PMC - PubMed
-
- Hillis GS, Zehr KJ, Williams AW, Schaff HV, Orzulak TA, Daly RC, Mullany CJ, Rodeheffer RJ, Oh JK. Outcome of patients with low ejection fraction undergoing coronary artery bypass grafting: renal function and mortality after 3.8 years. Circulation. 2006;114:I414–I419. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of heart failure with preserved ejection fraction in a population‐based study. N Engl J Med. 2006;355:260–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
