

Impact of Exercise Restriction on Arrhythmic Risk Among Patients With Arrhythmogenic Right Ventricular Cardiomyopathy
- PMID: 29909402
- PMCID: PMC6220537
- DOI: 10.1161/JAHA.118.008843
Impact of Exercise Restriction on Arrhythmic Risk Among Patients With Arrhythmogenic Right Ventricular Cardiomyopathy
Abstract
Background: Prior studies have shown a close link between exercise and development of arrhythmogenic right ventricular cardiomyopathy. How much exercise restriction reduces ventricular arrhythmia (VA), how genotype modifies its benefit, and whether it reduces risk sufficiently to defer implantable cardioverter-defibrillator (ICD) placement in arrhythmogenic right ventricular cardiomyopathy are unknown.
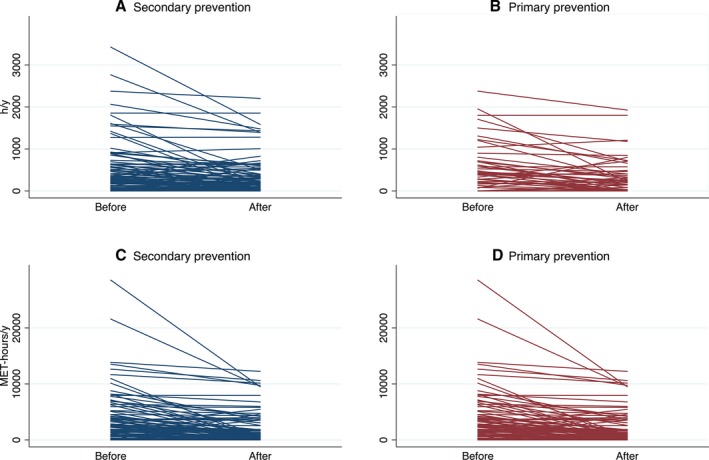
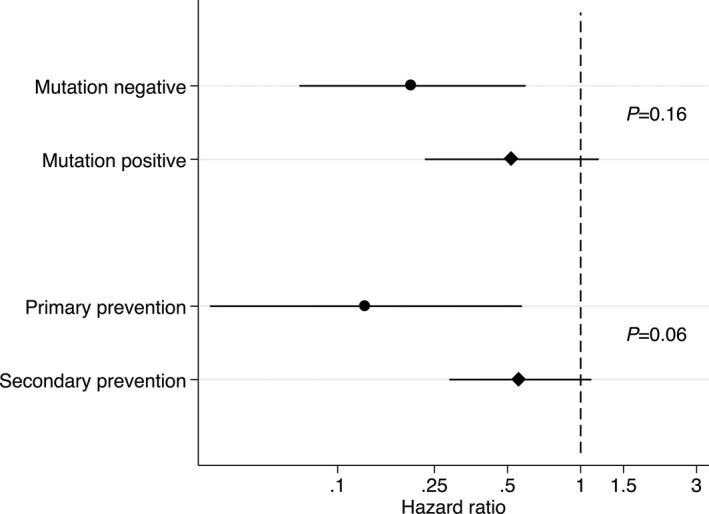
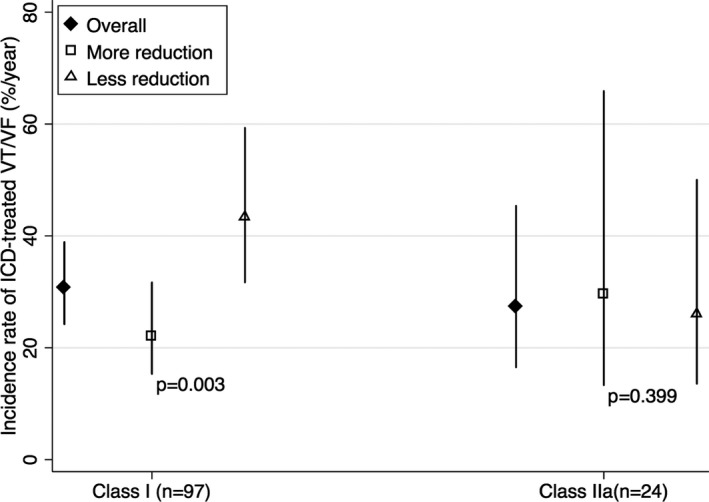
Methods and results: We interviewed 129 arrhythmogenic right ventricular cardiomyopathy patients (age: 34.0±14.8 years; male: 60%) with ICDs (36% primary prevention) about exercise participation. Exercise change was defined as annual exercise duration and dose in the 3 years before clinical presentation minus that after presentation. The primary outcome was appropriate ICD therapy for VA. During the 5.1 years (interquartile range: 2.7-10.8 years) after presentation, 74% (95/129) patients reduced exercise dose and 85 (66%) patients experienced the primary outcome. In multivariate analyses, top tertile reduction in exercise duration and dose were both associated with less VA (duration: hazard ratio: 0.23 [95% confidence interval, 0.07-0.81]; dose: hazard ratio: 0.14 [95% confidence interval, 0.04-0.44]). Greater reduction in exercise dose conferred greater reduction in VA (P=0.01 for trend). Patients without desmosomal mutations and those with primary-prevention ICDs benefited more from exercise reduction (P=0.16 and P=0.06 for interaction); however, 58% (18/31) of athletes who reduced exercise dose by >80% still experienced VA.
Conclusions: Exercise restriction should be recommended to all arrhythmogenic right ventricular cardiomyopathy patients with ICDs. Patients who are "gene-elusive" and those with primary-prevention devices may particularly benefit. Exercise reduction is unlikely to reduce arrhythmia sufficiently in high-risk patients to alter decision-making regarding ICD implantation.
Keywords: arrhythmogenic right ventricular cardiomyopathy; exercise; implantable cardioverter‐defibrillator; ventricular tachycardia.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Comment in
-
Exercise: A Risky Subject in Arrhythmogenic Cardiomyopathy.J Am Heart Assoc. 2018 Jun 16;7(12):e009611. doi: 10.1161/JAHA.118.009611. J Am Heart Assoc. 2018. PMID: 29909403 Free PMC article. No abstract available.
References
-
- Corrado D, Wichter T, Link MS, Hauer R, Marchlinski F, Anastasakis A, Bauce B, Basso C, Brunckhorst C, Tsatsopoulou A, Tandri H, Paul M, Schmied C, Pelliccia A, Duru F, Protonotarios N, Estes NA III, McKenna WJ, Thiene G, Marcus FI, Calkins H. Treatment of arrhythmogenic right ventricular cardiomyopathy/dysplasia: an international task force consensus statement. Eur Heart J. 2015;36:3227–3237. - PMC - PubMed
-
- James CA, Bhonsale A, Tichnell C, Murray B, Russell SD, Tandri H, Tedford RJ, Judge DP, Calkins H. Exercise increases age‐related penetrance and arrhythmic risk in arrhythmogenic right ventricular dysplasia/cardiomyopathy–associated desmosomal mutation carriers. J Am Coll Cardiol. 2013;62:1290–1297. - PMC - PubMed
-
- Saberniak J, Hasselberg NE, Borgquist R, Platonov PG, Sarvari SI, Smith H‐J, Ribe M, Holst AG, Edvardsen T, Haugaa KH. Vigorous physical activity impairs myocardial function in patients with arrhythmogenic right ventricular cardiomyopathy and in mutation positive family members. Eur J Heart Fail. 2014;16:1337–1344. - PMC - PubMed
-
- Sawant AC, Bhonsale A, te Riele AS, Tichnell C, Murray B, Russell SD, Tandri H, Tedford RJ, Judge DP, Calkins H. Exercise has a disproportionate role in the pathogenesis of arrhythmogenic right ventricular dysplasia/cardiomyopathy in patients without desmosomal mutations. J Am Heart Assoc. 2014;3:e001471 DOI: 10.1161/JAHA.114.001471. - DOI - PMC - PubMed
-
- La Gerche A, Robberecht C, Kuiperi C, Nuyens D, Willems R, de Ravel T, Matthijs G, Heidbüchel H. Lower than expected desmosomal gene mutation prevalence in endurance athletes with complex ventricular arrhythmias of right ventricular origin. Heart. 2010;96:1268–1274. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
