

Impact of surgical pulmonary valve replacement on ventricular strain and synchrony in patients with repaired tetralogy of Fallot: a cardiovascular magnetic resonance feature tracking study
- PMID: 29909772
- PMCID: PMC6004693
- DOI: 10.1186/s12968-018-0460-0
Impact of surgical pulmonary valve replacement on ventricular strain and synchrony in patients with repaired tetralogy of Fallot: a cardiovascular magnetic resonance feature tracking study
Abstract
Background: In patients with repaired tetralogy of Fallot (TOF), a better understanding of the impact of surgical pulmonary valve replacement (PVR) on ventricular mechanics may lead to improved indications and outcomes. Therefore, we used cardiovascular magnetic resonance (CMR) feature tracking analysis to quantify ventricular strain and synchrony in repaired TOF patients before and after PVR.
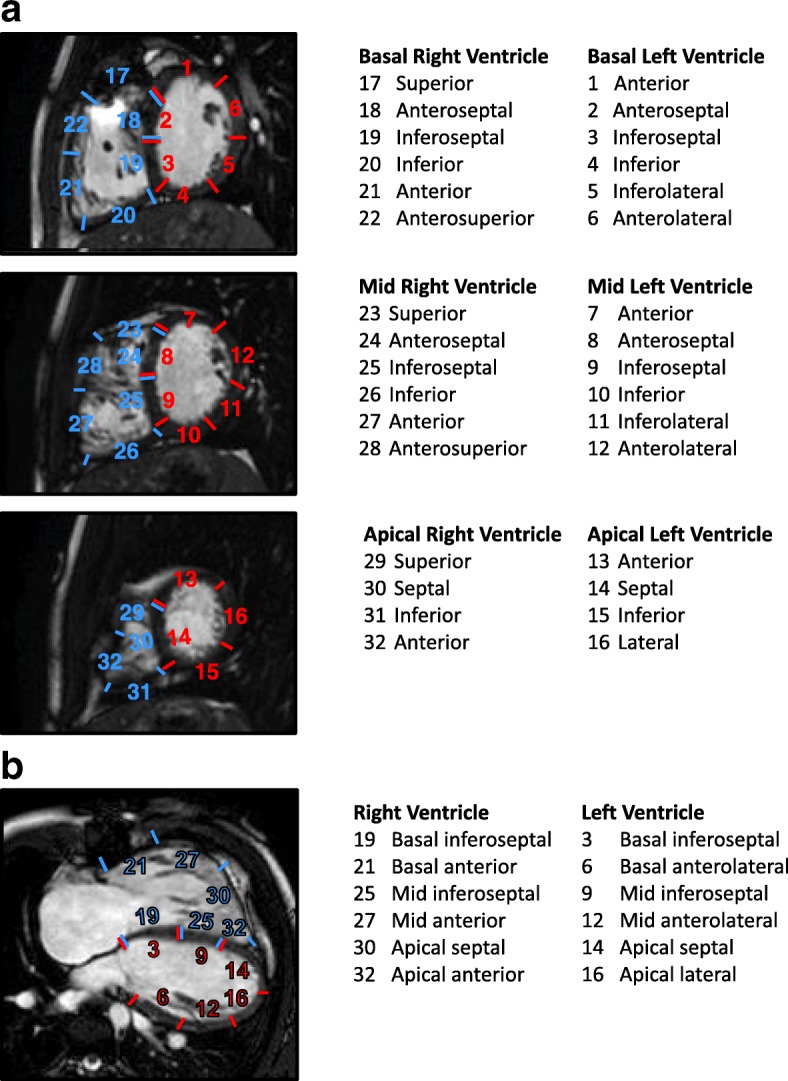
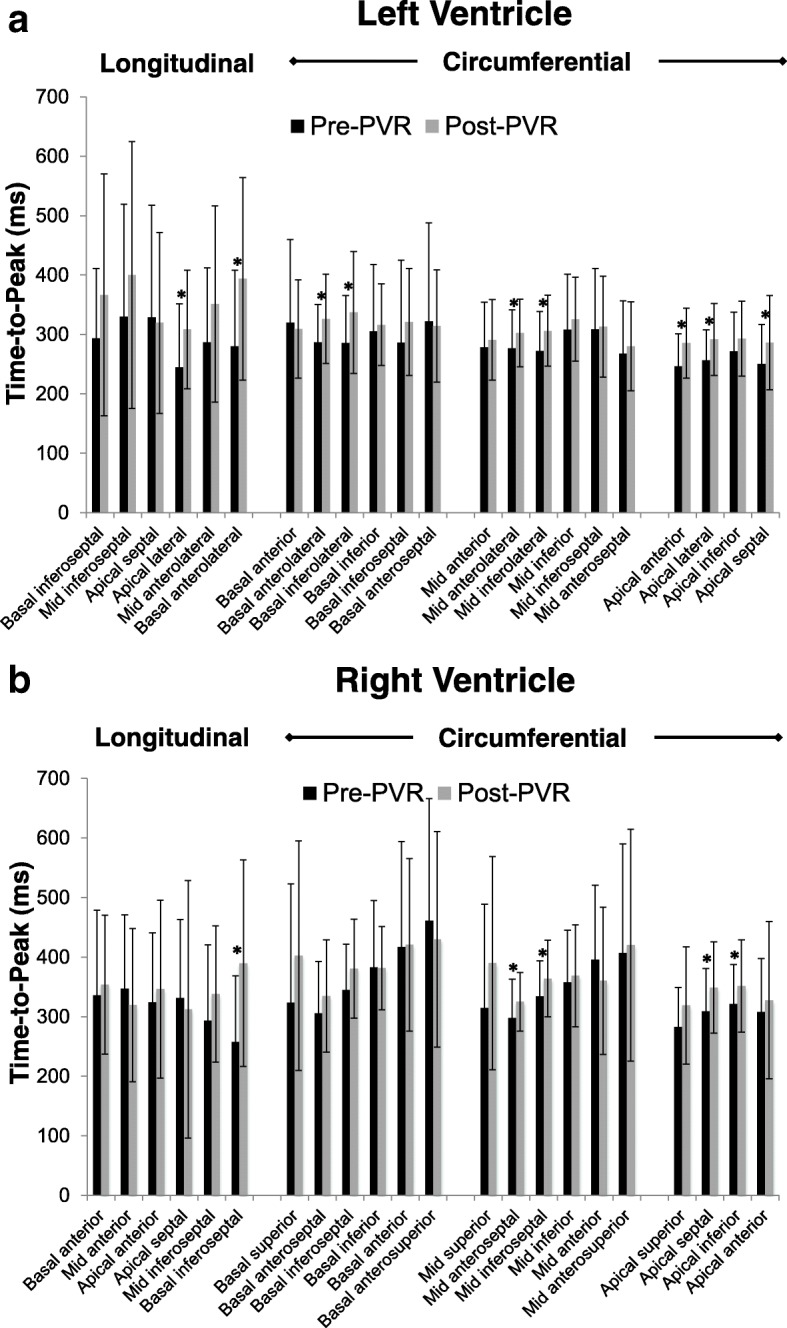
Methods: Thirty-six repaired TOF patients (median age 22.4 years) prospectively underwent CMR a mean of 4.5 ± 3.8 months before PVR surgery and 7.3 ± 2.1 months after PVR surgery. Feature tracking analysis on cine steady-state free precession images was used to measure right ventricular (RV) and left ventricular (LV) circumferential strain from short-axis views at basal, mid-ventricular, and apical levels; and longitudinal strain from 4-chamber views. Intraventricular synchrony was quantified using the maximum difference in time-to-peak strain, the standard deviation of the time-to-peak, and cross correlation delay (CCD) metrics; interventricular synchrony was assessed using the CCD metric.
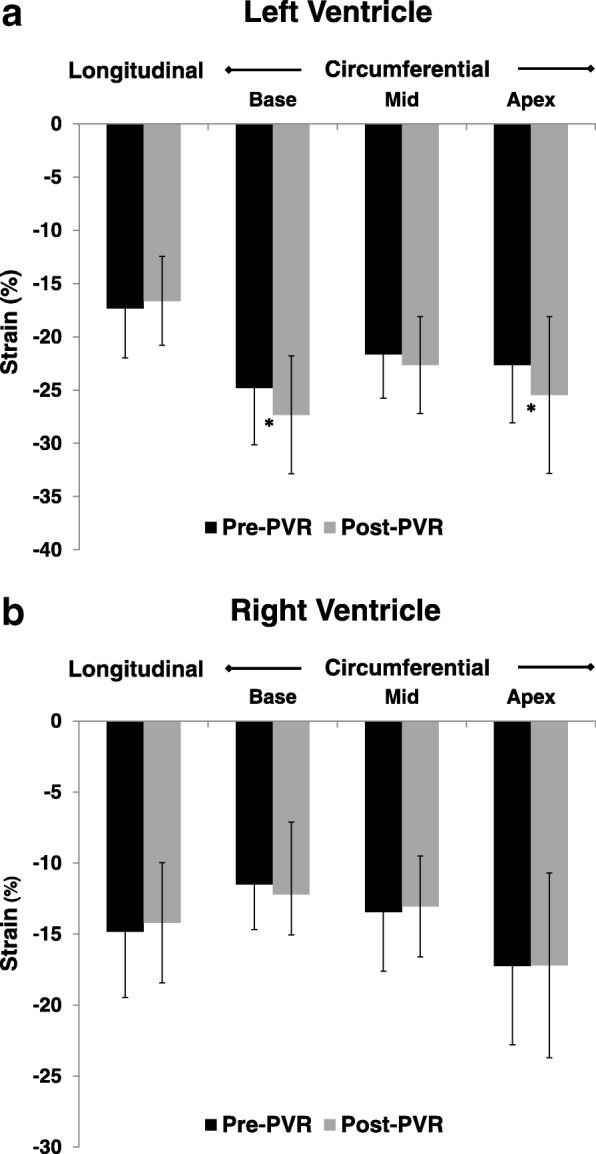
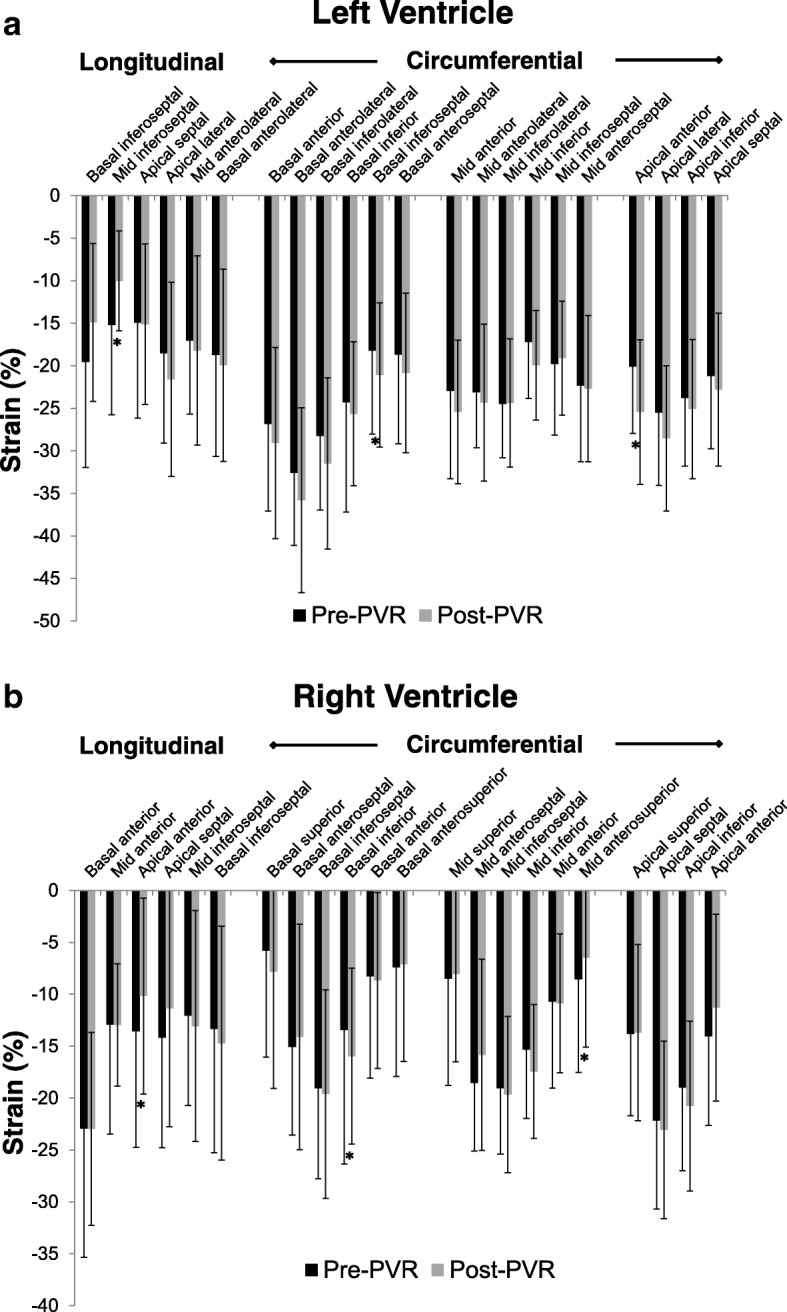
Results: Following PVR, RV end-diastolic volume, end-systolic volume, and ejection fraction declined, and LV end-diastolic volume and end-systolic volume both increased with no significant change in the LV ejection fraction. LV global basal and apical circumferential strains, and basal synchrony improved. RV global circumferential and longitudinal strains were unchanged, and there was a varied impact on synchrony across the locations. Interventricular synchrony worsened at the midventricular level but was unchanged at the base and apex, and on 4-chamber views.
Conclusions: Surgical PVR in repaired TOF patients led to improved LV global strain and no change in RV global strain. LV and RV synchrony parameters improved or were unchanged, and interventricular synchrony worsened at the midventricular level.
Keywords: Feature tracking; Myocardial strain; Pulmonary valve replacement; Tetralogy of fallot; Ventricular synchrony.
Conflict of interest statement
Ethics approval and consent to participate
The Boston Children’s Hospital Committee on Clinical Investigation granted permission for this study and waived the requirement for informed consent.
Competing interests
All authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Valente AM, Gauvreau K, Assenza GE, Babu-Narayan SV, Schreier J, Gatzoulis MA, et al. Contemporary predictors of death and sustained ventricular tachycardia in patients with repaired tetralogy of Fallot enrolled in the INDICATOR cohort. Heart. 2014;100(3):247–253. doi: 10.1136/heartjnl-2013-304958. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
