

Closure, Anticoagulation, or Antiplatelet Therapy for Cryptogenic Stroke With Patent Foramen Ovale: Systematic Review of Randomized Trials, Sequential Meta-Analysis, and New Insights From the CLOSE Study
- PMID: 29910193
- PMCID: PMC6220551
- DOI: 10.1161/JAHA.117.008356
Closure, Anticoagulation, or Antiplatelet Therapy for Cryptogenic Stroke With Patent Foramen Ovale: Systematic Review of Randomized Trials, Sequential Meta-Analysis, and New Insights From the CLOSE Study
Abstract
Background: We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing patent foramen ovale (PFO) closure, anticoagulation, and antiplatelet therapy to prevent stroke recurrence in patients with PFO-associated cryptogenic stroke.
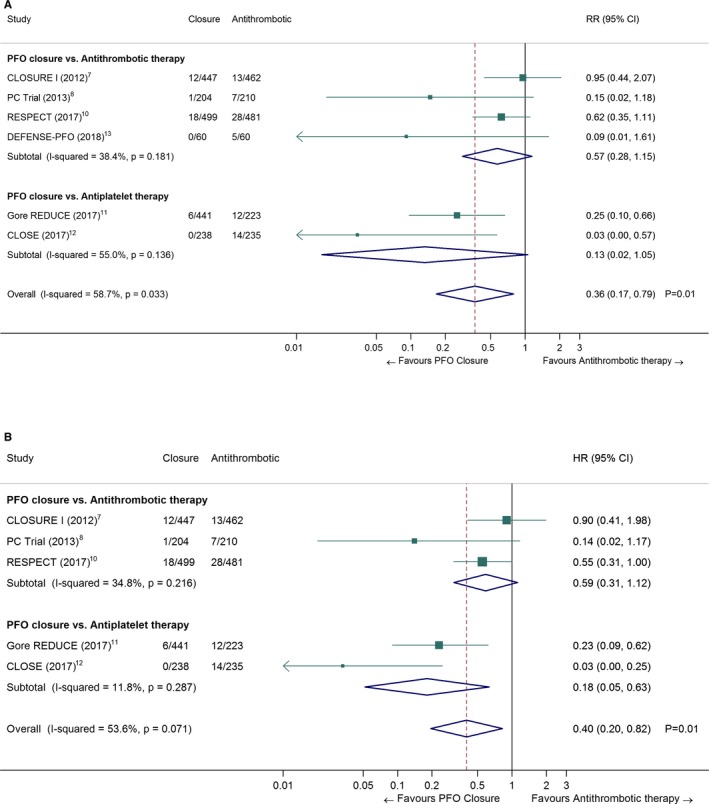
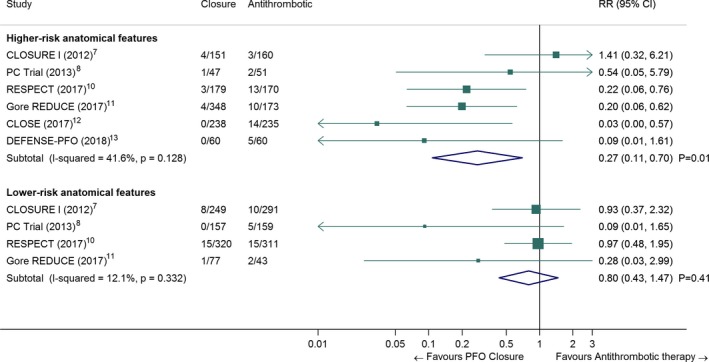
Methods and results: We searched Medline, Cochrane Library, and EMBASE through March 2018. The primary outcome was stroke recurrence. Pooled incidences, hazard ratios, and risk ratios (RRs) were calculated in random-effects meta-analyses. PFO closure was associated with a lower risk of recurrent stroke compared with antithrombotic therapy (antiplatelet therapy or anticoagulation: 3560 patients from 6 RCTs; RR=0.36, 95% CI: 0.17-0.79; I2=59%). The effect of PFO closure on stroke recurrence was larger in patients with atrial septal aneurysm or large shunt (RR=0.27, 95% CI, 0.11-0.70; I2=42%) compared with patients without these anatomical features (RR=0.80, 95% CI, 0.43-1.47; I2=12%). Major complications occurred in 2.40% (95% CI, 1.03-4.25; I2=77%) of procedures. New-onset atrial fibrillation was more frequent in patients randomized to PFO closure versus antithrombotic therapy (RR=4.33, 95% CI, 2.37-7.89; I2=14%). One RCT compared PFO closure versus anticoagulation (353 patients; hazard ratio=0.14, 95% CI, 0.00-1.45) and 2 RCTs compared PFO closure versus antiplatelet therapy (1137 patients; hazard ratio=0.18, 95% CI, 0.05-0.63; I2=12%). Three RCTs compared anticoagulation versus antiplatelet therapy, with none showing a significant difference.
Conclusions: PFO closure is superior to antithrombotic therapy to prevent stroke recurrence after cryptogenic stroke. The annual absolute risk reduction of stroke was low, but it has to be tempered by a substantial time at risk (at least 5 years) in young and middle-aged patients. PFO closure was associated with an increased risk of atrial fibrillation.
Trial registration: ClinicalTrials.gov NCT00562289.
Keywords: anticoagulation; patent foramen ovale; patent foramen ovale closure; stroke.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

Comment in
-
Odyssey of Patent Foramen Ovale: Closure in Cryptogenic Stroke: The Canary in the Coal Mine of Clinical Trials?J Am Heart Assoc. 2018 Jun 17;7(12):e009558. doi: 10.1161/JAHA.118.009558. J Am Heart Assoc. 2018. PMID: 29910194 Free PMC article. No abstract available.
References
-
- Sacco RL, Ellenberg JH, Mohr JP, Tatemichi TK, Hier DB, Price TR, Wolf PA. Infarcts of undetermined cause: the NINCDS Stroke Data Bank. Ann Neurol. 1989;25:382–390. - PubMed
-
- Hart RG, Diener HC, Coutts SB, Easton JD, Granger CB, O'Donnell MJ, Sacco RL, Connolly SJ; Cryptogenic Stroke EIWG . Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol. 2014;13:429–438. - PubMed
-
- Lechat P, Mas JL, Lascault G, Loron P, Theard M, Klimczac M, Drobinski G, Thomas D, Grosgogeat Y. Prevalence of patent foramen ovale in patients with stroke. N Engl J Med. 1988;318:1148–1152. - PubMed
-
- Kent DM, Ruthazer R, Weimar C, Mas JL, Serena J, Homma S, Di Angelantonio E, Di Tullio MR, Lutz JS, Elkind MS, Griffith J, Jaigobin C, Mattle HP, Michel P, Mono ML, Nedeltchev K, Papetti F, Thaler DE. An index to identify stroke‐related vs incidental patent foramen ovale in cryptogenic stroke. Neurology. 2013;81:619–625. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
