

Status of F-18 fluorodeoxyglucose uptake in normal and hibernating myocardium after glucose and insulin loading
- PMID: 29910577
- PMCID: PMC6000987
- DOI: 10.1016/j.jsha.2017.07.001
Status of F-18 fluorodeoxyglucose uptake in normal and hibernating myocardium after glucose and insulin loading
Abstract
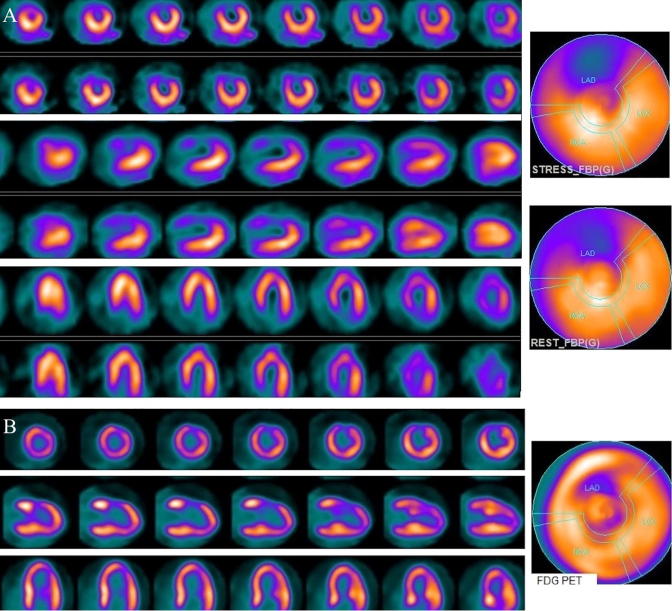
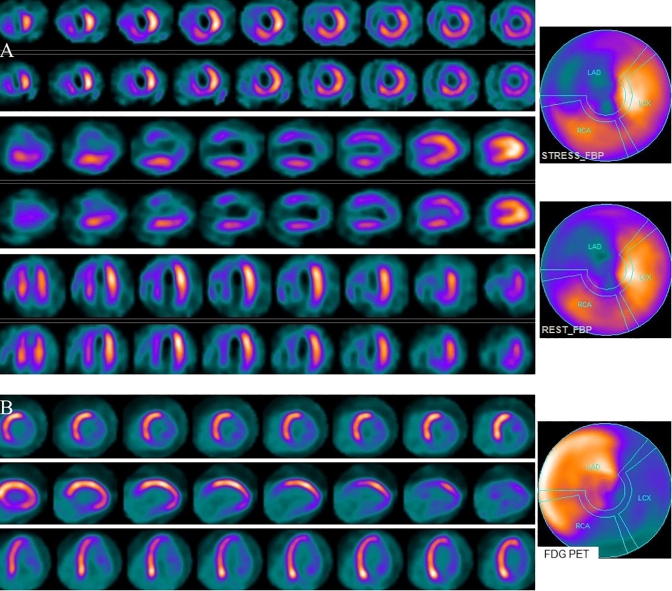
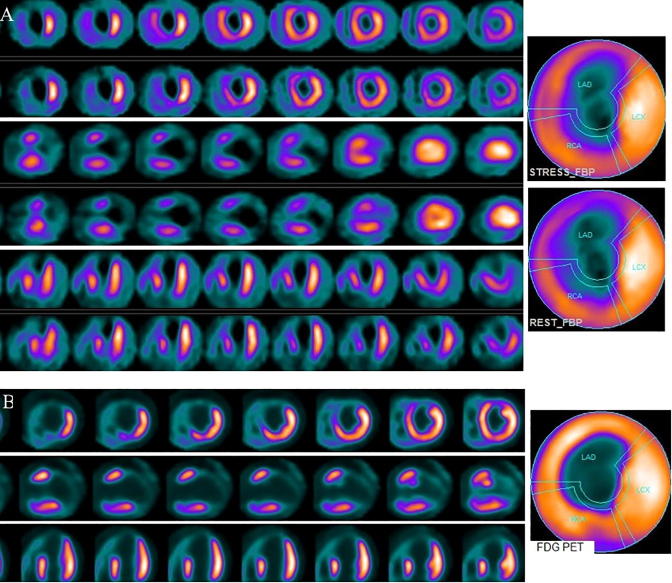
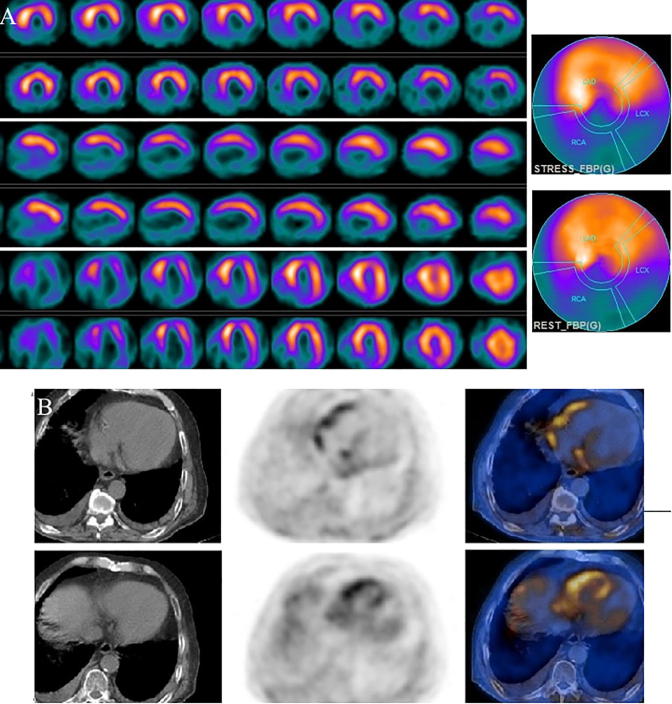
Objective: F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) has been increasingly used in myocardial viability imaging. In routine PET viability studies, oral glucose and intravenous insulin loading is commonly utilized. In an optimal study, glucose and insulin loading is expected to cause FDG uptake both in hibernating and normal myocardium. However, in routine studies it is not uncommon to see absent or reduced FDG uptake in normal myocardium. In this retrospective study we further analyzed our PET viability images to evaluate FDG uptake status in myocardium under the oral glucose and intravenous insulin loading protocol that we use in our hospital.
Methods: Patients who had both myocardial perfusion single photon emission computed tomography (SPECT) and FDG PET cardiac viability studies were selected for analysis. FDG uptake status in normal and abnormal myocardial segments on perfusion SPECT was evaluated. Based on SPECT and PET findings, patients were divided into two main groups and four subgroups. Group 1 included PET viable studies and Group 2 included PET-nonviable studies. Subgroups based on FDG uptake in normal myocardium were 1a and 2a (normal uptake) and 1b and 2b (absent or significantly reduced uptake).
Results: Seventy-one patients met the inclusion criteria. Forty-two patients were PET-viable and 29 were PET-nonviable. In 33 of 71 patients (46.4%) there was absent or significantly reduced FDG uptake in one or more normal myocardial segments, which was identified more in PET-viable than PET-nonviable patients (59.5% vs. 27.5%, p = 0.008). This finding was also more frequent in diabetic than nondiabetic patients (53% vs. 31.8%), but the difference was not significant (p = 0.160).
Conclusions: In nearly half of our patients, one or more normal myocardial segments showed absent or significantly reduced FDG uptake. This finding, particularly if it is diffuse, could be from suboptimal study, inadequacy of current glucose and insulin loading protocols, or various other patient-related causes affecting FDG uptake both in the normal and hibernating myocardium. In cases with significantly reduced FDG uptake in normal myocardium, PET images should be interpreted cautiously to prevent false-negative results for viability.
Keywords: Fluorodeoxyglucose; Glucose loading; Insulin loading; Myocardial viability; Positron emission tomography.
Figures
Similar articles
-
Assessing oral glucose and intravenous insulin loading protocol in 18F-fluorodeoxyglucose positron emission tomography cardiac viability studies.World J Nucl Med. 2020 Feb 27;19(1):1-7. doi: 10.4103/wjnm.WJNM_58_18. eCollection 2020 Jan-Mar. World J Nucl Med. 2020. PMID: 32190015 Free PMC article.
-
Positron emission tomography for the assessment of myocardial viability: an evidence-based analysis.Ont Health Technol Assess Ser. 2005;5(16):1-167. Epub 2005 Oct 1. Ont Health Technol Assess Ser. 2005. PMID: 23074467 Free PMC article.
-
Low-carbohydrate diet versus euglycemic hyperinsulinemic clamp for the assessment of myocardial viability with 18F-fluorodeoxyglucose-PET: a pilot study.Int J Cardiovasc Imaging. 2014 Feb;30(2):415-23. doi: 10.1007/s10554-013-0324-5. Epub 2013 Nov 20. Int J Cardiovasc Imaging. 2014. PMID: 24253855
-
Acquisition, Processing, and Interpretation of PET 18F-FDG Viability and Inflammation Studies.Curr Cardiol Rep. 2021 Jul 16;23(9):124. doi: 10.1007/s11886-021-01555-7. Curr Cardiol Rep. 2021. PMID: 34269917 Review.
-
18-Fluorodeoxyglucose imaging with positron emission tomography and single photon emission computed tomography: cardiac applications.Semin Nucl Med. 2000 Oct;30(4):281-98. doi: 10.1053/snuc.2000.9543. Semin Nucl Med. 2000. PMID: 11105929 Review.
Cited by
-
Molecular imaging of myogenic stem/progenitor cells with [18F]-FHBG PET/CT system in SCID mice model of post-infarction heart.Sci Rep. 2021 Oct 6;11(1):19825. doi: 10.1038/s41598-021-98861-5. Sci Rep. 2021. PMID: 34615887 Free PMC article.
-
Applications of PET-MR Imaging in Cardiovascular Disorders.PET Clin. 2020 Oct;15(4):509-520. doi: 10.1016/j.cpet.2020.06.007. Epub 2020 Jul 21. PET Clin. 2020. PMID: 32888548 Free PMC article. Review.
-
Assessing oral glucose and intravenous insulin loading protocol in 18F-fluorodeoxyglucose positron emission tomography cardiac viability studies.World J Nucl Med. 2020 Feb 27;19(1):1-7. doi: 10.4103/wjnm.WJNM_58_18. eCollection 2020 Jan-Mar. World J Nucl Med. 2020. PMID: 32190015 Free PMC article.
References
-
- Schinkel A.F., Bax J.J., Poldermans D., Elhendy A., Ferrari R., Rahimtoola S.H. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32:375–410. - PubMed
-
- Bonow R.O., Dilsizian V. Thallium 201 for assessment of myocardial viability. Semin Nucl Med. 1991;21:230–241. - PubMed
-
- Knuuti M.J., Nuutila P., Ruotsalainen U., Saraste M., Härkönen R., Ahonen A. Euglycemic hyperinsulinemic clamp and oral glucose load in stimulating myocardial glucose utilization during positron emission tomography. J Nucl Med. 1992;33:1255–1262. - PubMed
-
- Marshall R.C., Tillisch J.H., Phelps M.E., Huang S.C., Carson R., Henze E. Identification and differentiation of resting myocardial ischemia and infarction in man with positron computed tomography, 18 F-labeled fluorodeoxyglucose and N-13 ammonia. Circulation. 1983;67:766–778. - PubMed
-
- Tillisch J., Brunken R., Marshall R., Schwaiger M., Mandelkern M., Phelps M. Reversibility of cardiac wall-motion abnormalities predicted by positron tomography. N Engl J Med. 1986;314:884–888. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
