

Circulating Vitamin D and Colorectal Cancer Risk: An International Pooling Project of 17 Cohorts
- PMID: 29912394
- PMCID: PMC6376911
- DOI: 10.1093/jnci/djy087
Circulating Vitamin D and Colorectal Cancer Risk: An International Pooling Project of 17 Cohorts
Abstract
Background: Experimental and epidemiological studies suggest a protective role for vitamin D in colorectal carcinogenesis, but evidence is inconclusive. Circulating 25-hydroxyvitamin D (25(OH)D) concentrations that minimize risk are unknown. Current Institute of Medicine (IOM) vitamin D guidance is based solely on bone health.
Methods: We pooled participant-level data from 17 cohorts, comprising 5706 colorectal cancer case participants and 7107 control participants with a wide range of circulating 25(OH)D concentrations. For 30.1% of participants, 25(OH)D was newly measured. Previously measured 25(OH)D was calibrated to the same assay to permit estimating risk by absolute concentrations. Study-specific relative risks (RRs) for prediagnostic season-standardized 25(OH)D concentrations were calculated using conditional logistic regression and pooled using random effects models.
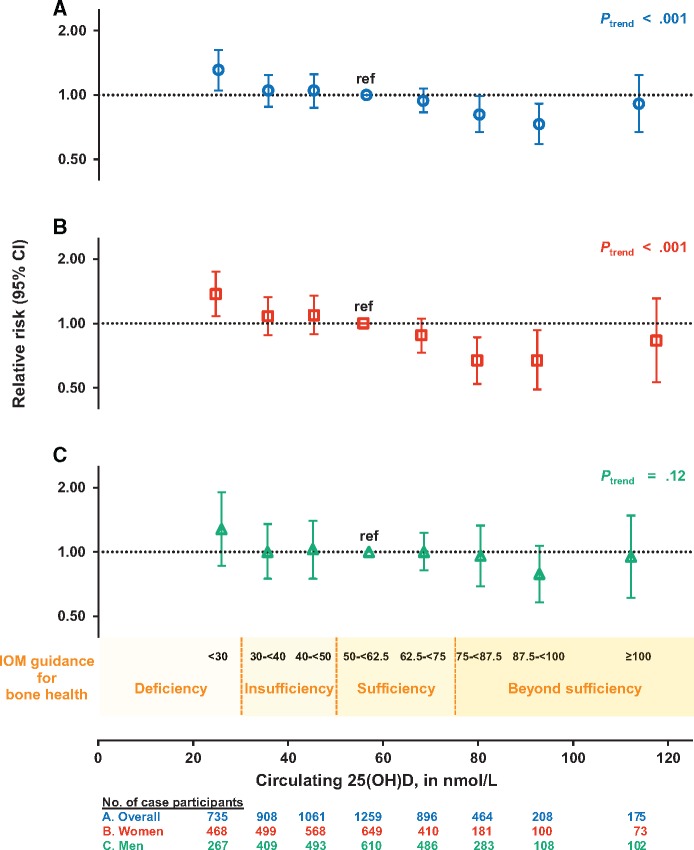
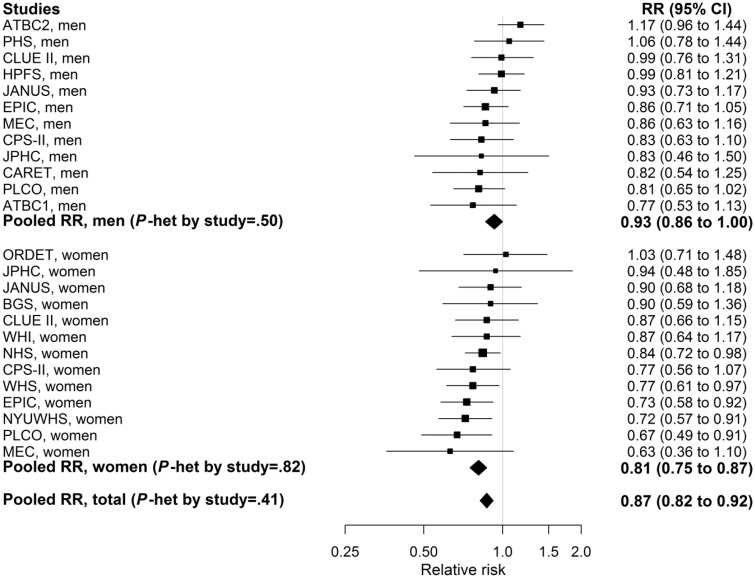
Results: Compared with the lower range of sufficiency for bone health (50-<62.5 nmol/L), deficient 25(OH)D (<30 nmol/L) was associated with 31% higher colorectal cancer risk (RR = 1.31, 95% confidence interval [CI] = 1.05 to 1.62); 25(OH)D above sufficiency (75-<87.5 and 87.5-<100 nmol/L) was associated with 19% (RR = 0.81, 95% CI = 0.67 to 0.99) and 27% (RR = 0.73, 95% CI = 0.59 to 0.91) lower risk, respectively. At 25(OH)D of 100 nmol/L or greater, risk did not continue to decline and was not statistically significantly reduced (RR = 0.91, 95% CI = 0.67 to 1.24, 3.5% of control participants). Associations were minimally affected when adjusting for body mass index, physical activity, or other risk factors. For each 25 nmol/L increment in circulating 25(OH)D, colorectal cancer risk was 19% lower in women (RR = 0.81, 95% CI = 0.75 to 0.87) and 7% lower in men (RR = 0.93, 95% CI = 0.86 to 1.00) (two-sided Pheterogeneity by sex = .008). Associations were inverse in all subgroups, including colorectal subsite, geographic region, and season of blood collection.
Conclusions: Higher circulating 25(OH)D was related to a statistically significant, substantially lower colorectal cancer risk in women and non-statistically significant lower risk in men. Optimal 25(OH)D concentrations for colorectal cancer risk reduction, 75-100 nmol/L, appear higher than current IOM recommendations.
Published by Oxford University Press 2018.
Figures

References
-
- Feldman D, Krishnan AV, Swami S, et al. The role of vitamin D in reducing cancer risk and progression. Nat Rev Cancer. 2014;145:342–357. - PubMed
-
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Colorectal Cancer. 2017. wcrf.org/colorectal-cancer-2017.
-
- Sempos CT, Vesper HW, Phinney KW, et al. Vitamin D status as an international issue: National surveys and the problem of standardization. Scand J Clin Lab Invest Suppl. 2012;243:32–40. - PubMed
-
- Wactawski-Wende J, Kotchen JM, Anderson GL, et al. Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Eng J Med. 2006;3547:684–696. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
