

Evaluation of the GeneXpert MTB/RIF in patients with presumptive tuberculous meningitis
- PMID: 29912907
- PMCID: PMC6005529
- DOI: 10.1371/journal.pone.0198695
Evaluation of the GeneXpert MTB/RIF in patients with presumptive tuberculous meningitis
Abstract
Background: Meningitis caused by Mycobacterium tuberculosis is a major cause of morbidity and mortality worldwide. We evaluated the performance of cerebrospinal fluid (CSF) testing with the GeneXpert MTB/RIF assay versus traditional approaches for diagnosing tuberculosis meningitis (TBM).
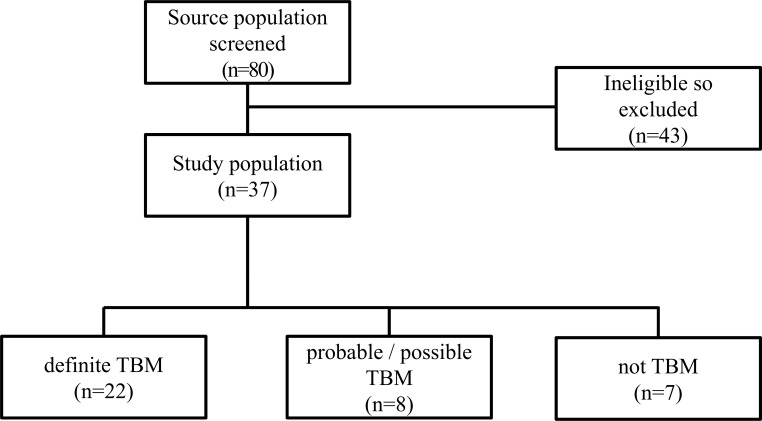
Methods: Patients were adults (n = 37) presenting with suspected TBM to the Hospital Nacional Dos de Mayo, Lima, Peru, during 12 months until 1st January 2015. Each participant had a single CSF specimen that was divided into aliquots that were concurrently tested for M. tuberculosis using GeneXpert, Ziehl-Neelsen smear and culture on solid and liquid media. Drug susceptibility testing used Mycobacteria Growth Indicator Tube (MGIT 960) and the proportions method.
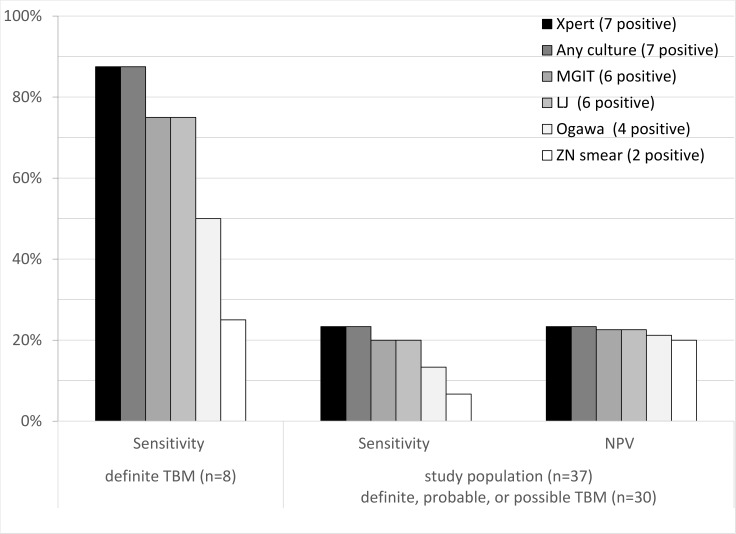
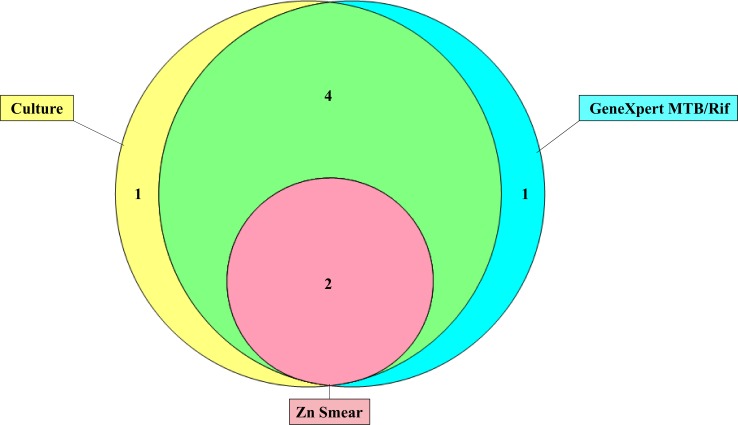
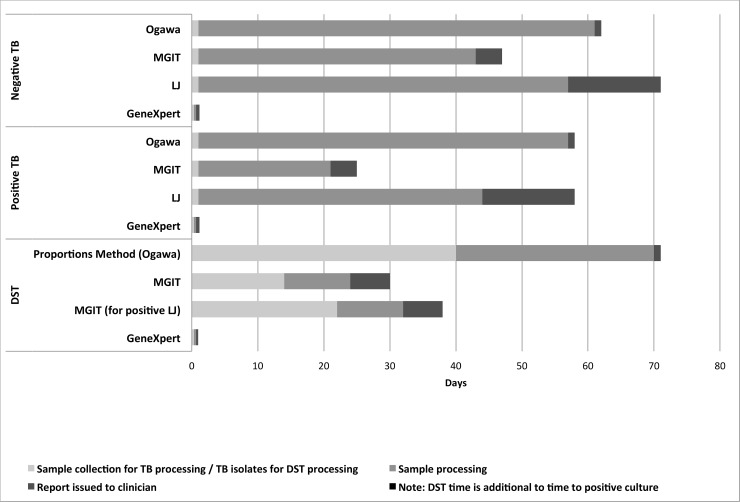
Results: 81% (30/37) of patients received a final clinical diagnosis of TBM, of whom 63% (19/30, 95% confidence intervals, CI: 44-80%) were HIV-positive. 22% (8/37, 95%CI: 9.8-38%), of patients had definite TBM. Because definite TBM was defined by positivity in any laboratory test, all laboratory tests had 100% specificity. Considering the 30 patients who had a clinical diagnosis of TBM: diagnostic sensitivity was 23% (7/30, 95%CI: 9.9-42%) for GeneXpert and was the same for all culture results combined; considerably greater than 7% (2/30, 95%CI: 0.82-22%) for microscopy; whereas all laboratory tests had poor negative predictive values (20-23%). Considering only the 8 patients with definite TBM: diagnostic sensitivity was 88% (7/8, 95%CI: 47-100%) for GeneXpert; 75% (6/8, 95%CI: 35-97%) for MGIT culture or LJ culture; 50% (4/8, 95%CI 16-84) for Ogawa culture and 25% (2/8, 95%CI: 3.2-65%) for microscopy. GeneXpert and microscopy provided same-day results, whereas culture took 20-56 days. GeneXpert provided same-day rifampicin-susceptibility results, whereas culture-based testing took 32-71 days. 38% (3/8, 95%CI: 8.5-76%) of patients with definite TBM with data had evidence of drug-resistant TB, but 73% (22/30) of all clinically diagnosed TBM (definite, probable, and possible TBM) had no drug-susceptibility results available.
Conclusions: Compared with traditional culture-based methods of CSF testing, GeneXpert had similar yield and faster results for both the detection of M. tuberculosis and drug-susceptibility testing. Including use of the GeneXpert has the capacity to improve the diagnosis of TBM cases.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. The top 10 causes of death factsheet– 2017 Geneva: WHO, 2017.
-
- Berenguer J, Moreno S, Laguna F, Vicente T, Adrados M, Ortega A, et al. Tuberculous meningitis in patients infected with the human immunodeficiency virus. N Engl J Med.1992; 326(10):668–72. doi: 10.1056/NEJM199203053261004 - DOI - PubMed
-
- Kingkaew N, Sangtong B, Amnuaiphon W, Jongpaibulpatana J, Mankatittham W, Akksilp S, et al. HIV-associated extrapulmonary tuberculosis in Thailand: epidemiology and risk factors for death. Int J Infect Dis. 2009; 13(6):722–9. doi: 10.1016/j.ijid.2008.11.013 - DOI - PubMed
-
- Marais S, Thwaites G, Schoeman JF, Torok ME, Misra UK, Prasad K, et al. Tuberculous meningitis: a uniform case definition for use in clinical research. Lancet Infect Dis. 2010; 10(11):803–12. doi: 10.1016/S1473-3099(10)70138-9 - DOI - PubMed
-
- Thwaites GE, Duc Bang N, Huy Dung N, Thi Quy H, Thi Tuong Oanh D, Thi Cam Thoa N, et al. The influence of HIV infection on clinical presentation, response to treatment, and outcome in adults with Tuberculous meningitis. J Infect Dis. 2005; 192(12):2134–41. doi: 10.1086/498220 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
