

Early mortality among children and adults in antiretroviral therapy programs in Southwest Ethiopia, 2003-15
- PMID: 29912974
- PMCID: PMC6005574
- DOI: 10.1371/journal.pone.0198815
Early mortality among children and adults in antiretroviral therapy programs in Southwest Ethiopia, 2003-15
Abstract
Background: Several studies reported that the majority of deaths in HIV-infected people are documented in their early antiretroviral therapy (ART) follow-ups. Early mortality refers to death of people on ART for follow up period of below 24 months due to any cause. The current study assessed predictors of early HIV mortality in Southwest Ethiopia.
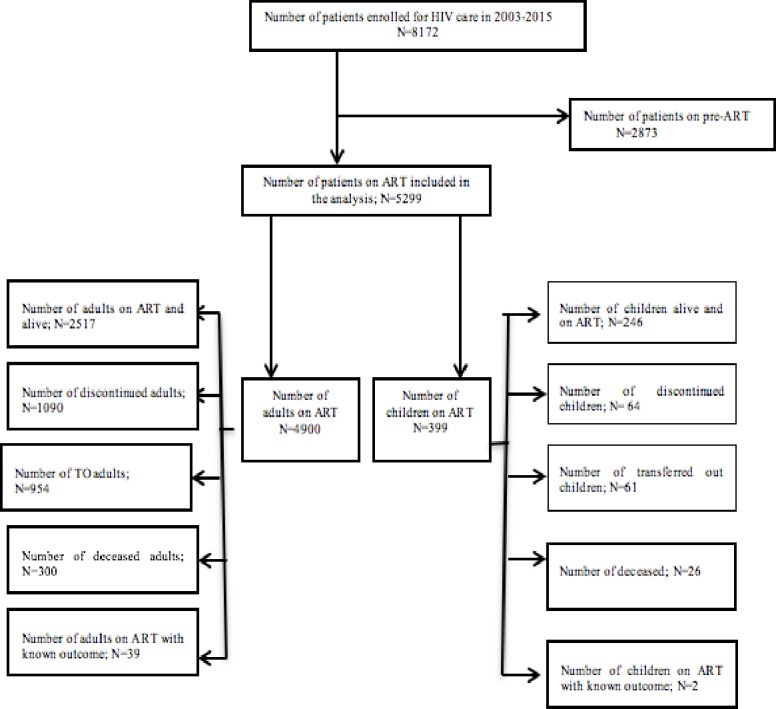
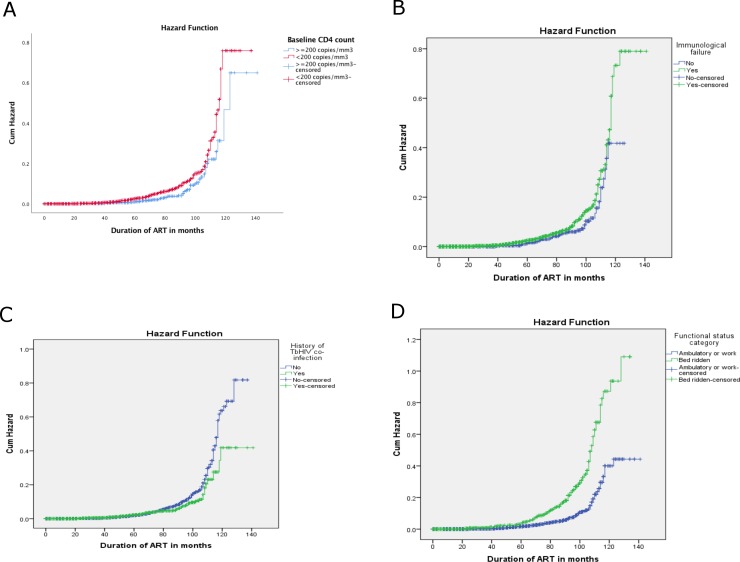
Methods: We have conducted a retrospective analysis of 5299 patient records dating from June 2003- March 2015. To estimate survival time and compare the time to event among the different groups of patients, we used a Kaplan Meir curve and log-rank test. To identify mortality predictors, we used a cox regression analysis. We used SPSS-20 for all analyses.
Results: A total of 326 patients died in the 12 years follow-up period contributing to 6.2% cumulative incidence and 21.7 deaths per 1000 person-year observations incidence rate. Eighty-nine percent of the total deaths were documented in the first two years follow up-an early-term ART follow up. Early HIV mortality rates among adults were 50% less in separated, divorced or widowed patients compared with never married patients, 1.6 times higher in patients with baseline CD4 count <200 cells/μL compared to baseline CD4 count ≥200 cells/μL, 1.5 times higher in patients with baseline WHO clinical stage 3 or 4 compared to baseline WHO clinical stage 1 or 2, 2.1 times higher in patients with immunologic failure compared with no immunologic failure, 60% less in patients with fair or poor compared with good adherence, 2.9 times higher in patients with bedridden functional status compared to working functional status, and 2.7 times higher with patients who had no history of HIV testing before diagnosis compared to those who had history of HIV testing. Most predictors of early mortality remained the same to the predictors of an overall HIV mortality. When discontinuation was assumed as an event, the predictors of an overall HIV mortality included age between 25-50 years, base line CD4 count, developing immunologic failure, bedridden functional status, and no history of HIV testing before diagnosis.
Conclusions: The great majority of deaths were documented in the first two years of ART, and several predictors of early HIV mortality were also for the overall mortality when discontinuation was assumed as event or censored. Considering the above population, interventions to improve HIV program in the first two years of ART follow up should be improved.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Wang H, Wolock TM, Carter A, Nguyen G, Kyu HH, Gakidou E, et al. Estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2015: the Global Burden of Disease Study 2015. Lancet HIV. 2016;3(8):e361–87. Epub 2016/07/30. doi: 10.1016/S2352-3018(16)30087-X . - DOI - PMC - PubMed
-
- UNAIDS. The gap report. Geneva, Switzerland: 2014.
-
- Mekonnen Yared, Rachel Sanders, Senait Tibebu, Emmart P. Equity and Access to ART in Ethiopia. USA: USAID, Initiative HP; 2010 2010. Report No.: 1.
-
- Mitiku H, Abdosh T, Teklemariam Z. Factors affecting adherence to antiretroviral treatment in harari national regional state, eastern ethiopia. Isrn aids. 2013;2013:960954 Epub 2013/09/21. doi: 10.1155/2013/960954 ; PubMed Central PMCID: PMCPmc3773384. - DOI - PMC - PubMed
-
- Assefa Y, Alebachew A, Lera M, Lynen L, Wouters E, Van Damme W. Scaling up antiretroviral treatment and improving patient retention in care: lessons from Ethiopia, 2005–2013. Globalization and Health. 2014;10:43–. doi: 10.1186/1744-8603-10-43 PubMed PMID: PMC4046386. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
