

The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation
- PMID: 29914186
- PMCID: PMC6023458
- DOI: 10.3390/dj6020021
The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation
Abstract
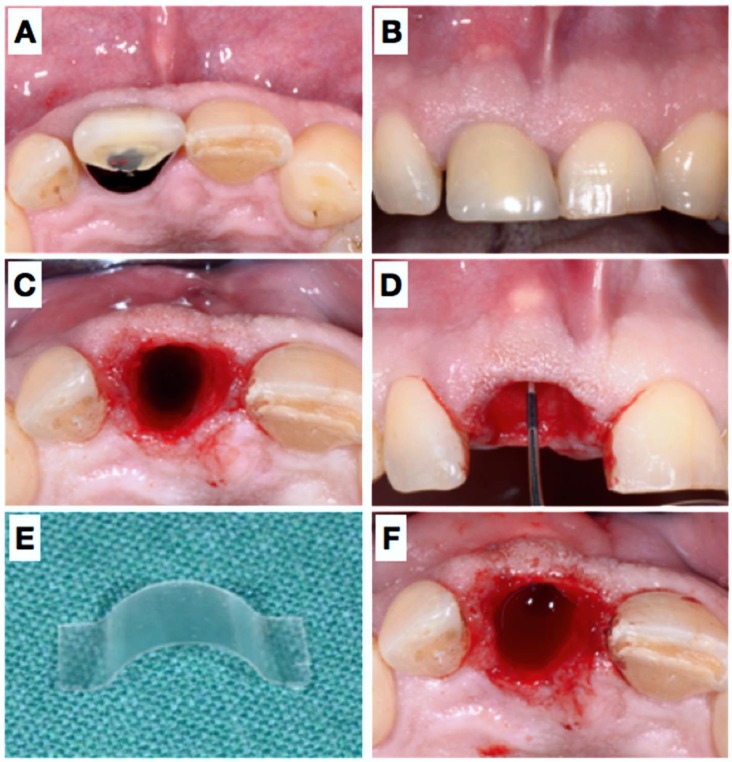
Tooth extraction causes vertical and horizontal alveolar bone loss and consequent remodeling. Several methods have been introduced in terms of so-called “ridge preservation” techniques, which mostly resemble guided bone regenerative (GBR) procedures using filler materials and membranes in order to stabilize the respective sites. This conceptual case report describes a novel approach using a degradable polylactic acid membrane covered with a collagen matrix, which aims to reshape the resorbed alveolar wall and thereby to stabilize the soft tissues during matrix formation and socket mineralization. Clinical re-entry, radiographic (CBCT) and histologic evaluation proved adequate for osteoneogenesis despite an unfavorable initial situation: An implant could be ideally placed, which was circumferentially covered by bone. This minimally invasive method could offer a new method to approach socket preservation without using filler materials and coverage of the socket entrance. However, more controlled research on this topic is needed.
Keywords: bone; dental implant; guided tissue regeneration; regeneration; ridge preservation; tooth extraction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






References
-
- Schmidlin P.R., Jung R.E., Schug J. Alveolarkammprävention nach Zahnextraktion-eine Literaturübersicht. Schweiz Monatsschr Zahnmed. 2004;114:328–336. - PubMed
-
- Lisowski C.S. A comparative study of the resorption of alveolar ridge tissue under immediate dentures. Dent. Res. Grad. Study. 1944;45:11–13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
