

Bioengineering Approaches for Bladder Regeneration
- PMID: 29914213
- PMCID: PMC6032229
- DOI: 10.3390/ijms19061796
Bioengineering Approaches for Bladder Regeneration
Abstract
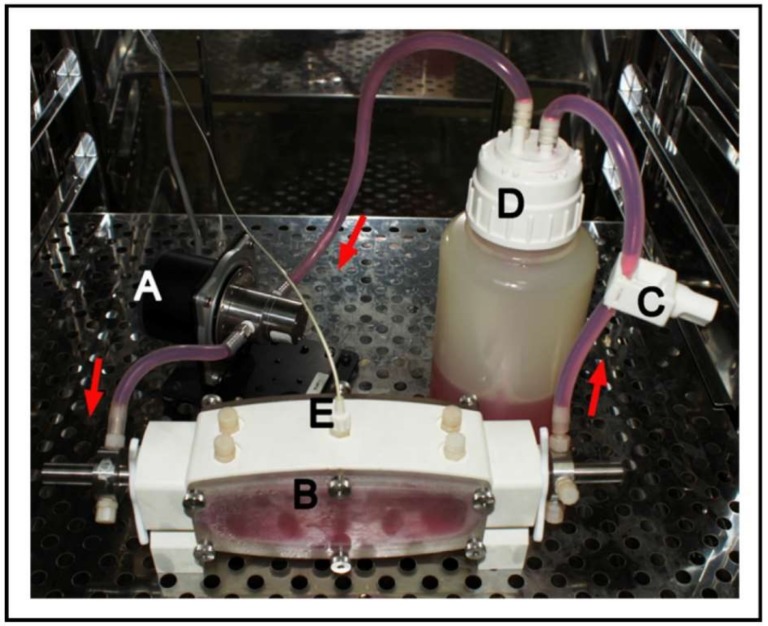
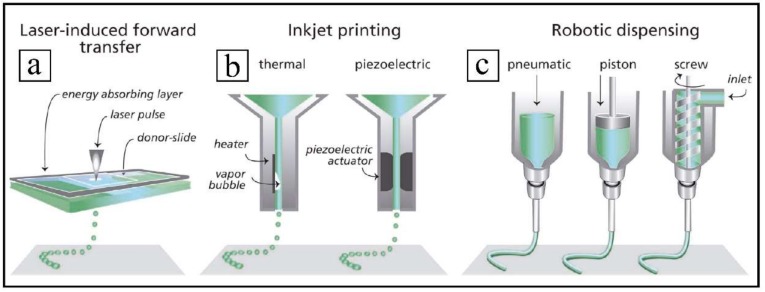
Current clinical strategies for bladder reconstruction or substitution are associated to serious problems. Therefore, new alternative approaches are becoming more and more necessary. The purpose of this work is to review the state of the art of the current bioengineering advances and obstacles reported in bladder regeneration. Tissue bladder engineering requires an ideal engineered bladder scaffold composed of a biocompatible material suitable to sustain the mechanical forces necessary for bladder filling and emptying. In addition, an engineered bladder needs to reconstruct a compliant muscular wall and a highly specialized urothelium, well-orchestrated under control of autonomic and sensory innervations. Bioreactors play a very important role allowing cell growth and specialization into a tissue-engineered vascular construct within a physiological environment. Bioprinting technology is rapidly progressing, achieving the generation of custom-made structural supports using an increasing number of different polymers as ink with a high capacity of reproducibility. Although many promising results have been achieved, few of them have been tested with clinical success. This lack of satisfactory applications is a good reason to discourage researchers in this field and explains, somehow, the limited high-impact scientific production in this area during the last decade, emphasizing that still much more progress is required before bioengineered bladders become a commonplace in the clinical setting.
Keywords: bioreactors; bladder regeneration; c; regenerative medicine; scaffolds; stem cells.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Bladder muscular wall regeneration with autologous adipose mesenchymal stem cells on three-dimensional collagen-based tissue-engineered prepuce and biocompatible nanofibrillar scaffold.J Pediatr Urol. 2014 Dec;10(6):1051-8. doi: 10.1016/j.jpurol.2014.03.010. Epub 2014 May 2. J Pediatr Urol. 2014. PMID: 24909608
-
Human urinary bladder regeneration through tissue engineering - an analysis of 131 clinical cases.Exp Biol Med (Maywood). 2014 Mar;239(3):264-71. doi: 10.1177/1535370213517615. Epub 2014 Jan 13. Exp Biol Med (Maywood). 2014. PMID: 24419462 Review.
-
Application of different scaffolds for bladder wall regeneration: the bladder as a natural bioreactor.Tissue Eng Part A. 2012 Apr;18(7-8):882-7. doi: 10.1089/ten.TEA.2011.0202. Epub 2012 Jan 5. Tissue Eng Part A. 2012. PMID: 22060916
-
Concise Review: Tissue Engineering of Urinary Bladder; We Still Have a Long Way to Go?Stem Cells Transl Med. 2017 Nov;6(11):2033-2043. doi: 10.1002/sctm.17-0101. Epub 2017 Oct 10. Stem Cells Transl Med. 2017. PMID: 29024555 Free PMC article. Review.
-
Current Applications and Future Directions of Bioengineering Approaches for Bladder Augmentation and Reconstruction.Front Surg. 2021 Jun 18;8:664404. doi: 10.3389/fsurg.2021.664404. eCollection 2021. Front Surg. 2021. PMID: 34222316 Free PMC article. Review.
Cited by
-
[Application and progress of bio-derived materials in bladder regeneration and repair].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Nov 15;38(11):1299-1306. doi: 10.7507/1002-1892.202404099. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 39542618 Free PMC article. Review. Chinese.
-
Fabrication of Surfactant-Dispersed HiPco Single-Walled Carbon Nanotube-Based Alginate Hydrogel Composites as Cellular Products.Int J Mol Sci. 2019 Sep 27;20(19):4802. doi: 10.3390/ijms20194802. Int J Mol Sci. 2019. PMID: 31569637 Free PMC article.
-
Preliminary In Vitro Assessment of Decellularized Porcine Descending Aorta for Clinical Purposes.J Funct Biomater. 2023 Mar 2;14(3):141. doi: 10.3390/jfb14030141. J Funct Biomater. 2023. PMID: 36976065 Free PMC article.
-
Urinary bladder reconstruction using autologous collagenous connective tissue membrane "Biosheet®" induced by in-body tissue architecture: A pilot study.Regen Ther. 2020 Nov 20;15:274-280. doi: 10.1016/j.reth.2020.10.006. eCollection 2020 Dec. Regen Ther. 2020. PMID: 33426229 Free PMC article.
-
Prx1 + and Hic1+ Mesenchymal Progenitors Are Present Within the Epidural Fat and Dura Mater and Participate in Dural Injury Repair.Stem Cells Transl Med. 2022 Mar 17;11(2):200-212. doi: 10.1093/stcltm/szab014. Stem Cells Transl Med. 2022. PMID: 35259263 Free PMC article.
References
-
- World Health Organization . GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012 v1.0. WHO; Geneva, Switzerland: 2012.
-
- Stenzl A., Nagele U., Kuczyk M., Sievert K.-D., Anastasiadis A., Seibold J., Corvin S. Cystectomy—Technical Considerations in Male and Female Patients. EAU Update Ser. 2005;3:138–146. doi: 10.1016/j.euus.2005.07.004. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
