

Early use of alendronate as a protective factor against the development of glucocorticoid-induced bone loss in childhood-onset rheumatic diseases: a cross-sectional study
- PMID: 29914510
- PMCID: PMC6006935
- DOI: 10.1186/s12969-018-0258-5
Early use of alendronate as a protective factor against the development of glucocorticoid-induced bone loss in childhood-onset rheumatic diseases: a cross-sectional study
Abstract
Background: Bisphosphonates are recommended for use as first-line therapy for the prevention and treatment of glucocorticoid-induced osteoporosis in adults. However, the appropriate usage of bisphosphonates for the prevention or treatment of glucocorticoid-induced osteoporosis in children remains unclear.
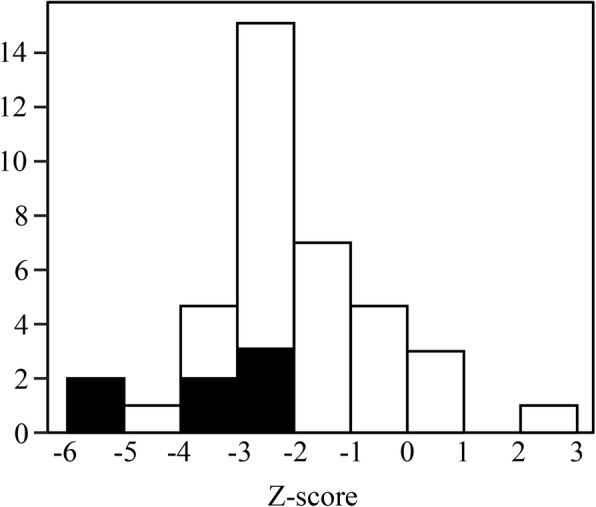
Methods: We performed a cross-sectional study to clarify the factors associated with the development of glucocorticoid-induced bone loss and osteoporosis in patients with childhood-onset rheumatic disease and to investigate the impact of the early use of alendronate. We recruited 39 patients with childhood-onset rheumatic disease who were evaluated to detect bone loss or osteoporosis at 3 months to 1.5 years after the initiation of treatment. The primary outcome of the study was the presence of bone loss or osteoporosis at the initial evaluation of the bone mineral density after at least 3 months of glucocorticoid therapy.
Results: Bone loss and a history of fracture were found in 56 and 18% of the participants, respectively. Weekly oral alendronate therapy (median, 25.4 mg/m2) had been started by the time of the evaluation of osteoporosis in 46% of the participants and within 3 months after the start of glucocorticoid in 31% of the participants. There were no significant differences between the participants with bone loss (wBL group) and without bone loss (w/oBL group) in terms of gender, primary disease, or the age at the onset of primary disease. In terms of glucocorticoid use, there was no significant difference in the age at the start of glucocorticoid therapy, the length of glucocorticoid use, or the dose of glucocorticoids. The proportion of patients in the w/oBL group who received alendronate within 3 months after the start of glucocorticoid therapy was significantly greater than that in the wBL group. In the logistic regression analysis, only "alendronate therapy within 3 months after the start of glucocorticoid therapy" had a statistically significant effect on the development of bone loss (OR, 0.08; 95% CI, 0.02-0.43). The analysis did not reveal any factors associated with the development of osteoporosis.
Conclusions: The early use of alendronate may have a preventive effect against the development of bone loss in glucocorticoid-treated patients with childhood-onset rheumatic disease.
Keywords: Alendronate; Bone loss; Childhood-onset rheumatic disease; Glucocorticoid; Osteoporosis.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Ethical Review Board of Chiba University Hospital (Approval number, 2887). Written informed consent was obtained from each of the study participants and their guardians.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- van Staa TP, Cooper C, Leufkens HGM, Bishop N. Children and the risk of fractures caused by oral corticosteroids. J Bone Miner Res [Internet]. 2003;18:913–918. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12733732 - PubMed
-
- Bonjour J-P, Chevalley T, Ferrari S, Rizzoli R. The importance and relevance of peak bone mass in the prevalence of osteoporosis. Salud Publica Mex [Internet]. 2009 [cited 2017 Dec 18];51 Suppl 1:S5–17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19287894 - PubMed
-
- Laan RF, van Riel PL, van de Putte LB, van Erning LJ, van’t Hof MA, Lemmens JA. Low-dose prednisone induces rapid reversible axial bone loss in patients with rheumatoid arthritis. A randomized, controlled study. Ann Intern Med [Internet]. 1993 [cited 2017 Dec 18];119:963–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8105737 - PubMed
-
- Buckley L, Guyatt G, Fink HA, Cannon M, Grossman J, Hansen KE, et al. 2017 American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Arthritis Care Res (Hoboken) [Internet]. 2017;69:1095–110. Available from: http://doi.wiley.com/10.1002/acr.23279 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
