

Reliability of LoSCAT score for activity and tissue damage assessment in a large cohort of patients with Juvenile Localized Scleroderma
- PMID: 29914516
- PMCID: PMC6006585
- DOI: 10.1186/s12969-018-0254-9
Reliability of LoSCAT score for activity and tissue damage assessment in a large cohort of patients with Juvenile Localized Scleroderma
Abstract
Objectives: To assess reliability of the two indexes of Localized Scleroderma Cutaneous Assessment Tool (LoSCAT), the modified Localized Scleroderma Skin Severity Index (mLoSSI) and the Localized Scleroderma Skin Damage Index (LoSDI), when applied by clinicians with different experience in scoring and managing patients with JLS. Secondary aim was to compare LoSCAT and infrared thermography (IRT) in monitoring lesions over time.
Methods: Consecutive children with Juvenile Localized Scleroderma (JLS) were blindly evaluated by three examiners with different experience in Paediatric Rheumatology and with no experience in LoSCAT use. At each visit, patients were assessed by LoSCAT and IRT. Sensitivity to change of LoSCAT and IRT was assessed in a group of patients 3-6 months later. Inter-rater reliability was assessed by Intraclass Correlation Coefficient (ICC) and variance analysis (ANOVA).
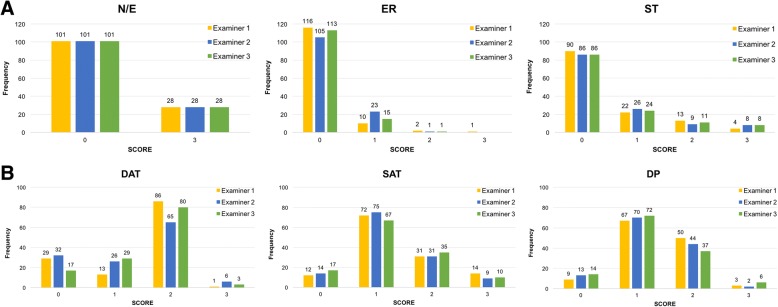
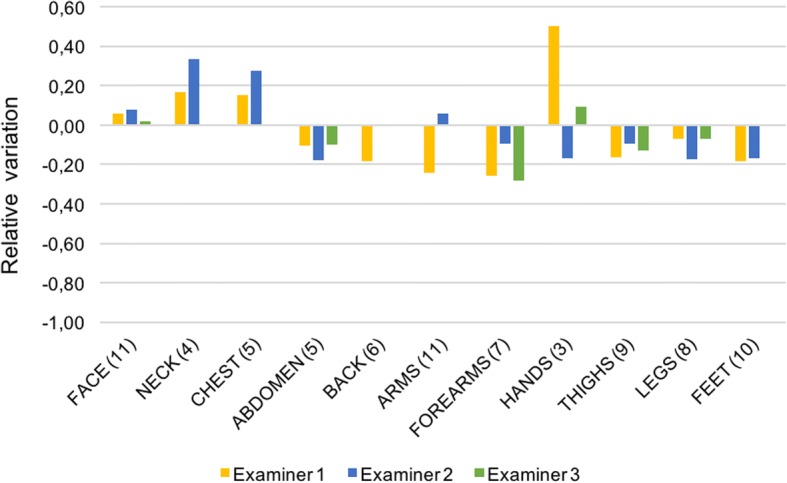
Findings: Forty-seven patients (129 lesions) entered the study, and 26 (79 lesions) were re-evaluated with same modality after 4.5 (SD 1.5) months. mLoSSI showed excellent inter-rater reliability expressed by ICC 0.965 confirmed by ANOVA. Similarly, inter-rater reliability for LoSDI was good (ICC = 0.774) but worse concordance among examiners was observed. A comparable improvement of mLoSSI in all anatomic sites was noted by all examiners in 79 lesions examined in two subsequent visits and was consistent with thermography.
Conclusions: Different clinical experience in JLS did not influence clinical judgement in mLoSSI which showed excellent concordance, whereas LoSDI is less precise in damage assessment and not completely reliable in monitoring skin changes. Infrared thermography confirms to be a helpful tool for detecting disease activity and reliable in monitoring lesions over time.
Keywords: Children; LoSCAT; Localized scleroderma; Morphea; Outcome measures; Thermography.
Conflict of interest statement
Ethics approval and consent to participate
No ethics approval was needed since LoSCAT and thermography are currently in use in the routine assessment of children with Localized Scleroderma. All participants gave their informed consent to participate.
Consent for publication
Obtained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
The Localized Scleroderma Cutaneous Assessment Tool: responsiveness to change in a pediatric clinical population.J Am Acad Dermatol. 2013 Aug;69(2):214-20. doi: 10.1016/j.jaad.2013.02.007. Epub 2013 Apr 4. J Am Acad Dermatol. 2013. PMID: 23562760 Free PMC article.
-
Localized Scleroderma Cutaneous Assessment Tool (LoSCAT) adapted for use in adult patients: report from an initial validation study.Health Qual Life Outcomes. 2018 Sep 14;16(1):185. doi: 10.1186/s12955-018-1010-z. Health Qual Life Outcomes. 2018. PMID: 30217204 Free PMC article.
-
Using the Localized Scleroderma Cutaneous Assessment Tool (LoSCAT) to classify morphoea by severity and identify clinically significant change.Br J Dermatol. 2020 Feb;182(2):398-404. doi: 10.1111/bjd.18097. Epub 2019 Aug 14. Br J Dermatol. 2020. PMID: 31049928
-
Disease course and long-term outcome of juvenile localized scleroderma: Experience from a single pediatric rheumatology Centre and literature review.Autoimmun Rev. 2018 Jul;17(7):727-734. doi: 10.1016/j.autrev.2018.02.004. Epub 2018 May 3. Autoimmun Rev. 2018. PMID: 29729451 Review.
-
New developments in juvenile systemic and localized scleroderma.Rheum Dis Clin North Am. 2013 Nov;39(4):905-20. doi: 10.1016/j.rdc.2013.05.003. Epub 2013 Jul 16. Rheum Dis Clin North Am. 2013. PMID: 24182860 Review.
Cited by
-
Why, how, and when to use color Doppler ultrasound for improving precision in the diagnosis, assessment of severity and activity in morphea.J Scleroderma Relat Disord. 2019 Feb;4(1):28-34. doi: 10.1177/2397198318799244. Epub 2018 Sep 24. J Scleroderma Relat Disord. 2019. PMID: 35382147 Free PMC article. Review.
-
Recent Advances in Treatment of Systemic Sclerosis and Morphea.Am J Clin Dermatol. 2024 Mar;25(2):213-226. doi: 10.1007/s40257-023-00831-2. Epub 2023 Dec 12. Am J Clin Dermatol. 2024. PMID: 38087156 Review.
-
National Registry for Childhood Onset Scleroderma I: Insights from the first 341 juvenile localized scleroderma patients.J Scleroderma Relat Disord. 2024 Sep 23:23971983241272460. doi: 10.1177/23971983241272460. Online ahead of print. J Scleroderma Relat Disord. 2024. PMID: 39544906 Free PMC article.
-
Clinical Application of Infrared Thermography in Rheumatic Diseases: A Systematic Review.Mediterr J Rheumatol. 2025 Jan 30;36(2):159-192. doi: 10.31138/mjr.271024.ita. eCollection 2025 Jun. Mediterr J Rheumatol. 2025. PMID: 40757122 Free PMC article.
-
Comparison of 3D facial photographs and clinical documentation in patients with craniofacial morphea.Skin Health Dis. 2024 Aug 10;4(6):e438. doi: 10.1002/ski2.438. eCollection 2024 Dec. Skin Health Dis. 2024. PMID: 39624764 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
