

Progression of Hypertrophy and Myocardial Fibrosis in Aortic Stenosis: A Multicenter Cardiac Magnetic Resonance Study
- PMID: 29914867
- PMCID: PMC6023592
- DOI: 10.1161/CIRCIMAGING.117.007451
Progression of Hypertrophy and Myocardial Fibrosis in Aortic Stenosis: A Multicenter Cardiac Magnetic Resonance Study
Abstract
Background: Aortic stenosis is accompanied by progressive left ventricular hypertrophy and fibrosis. We investigated the natural history of these processes in asymptomatic patients and their potential reversal post-aortic valve replacement (AVR).
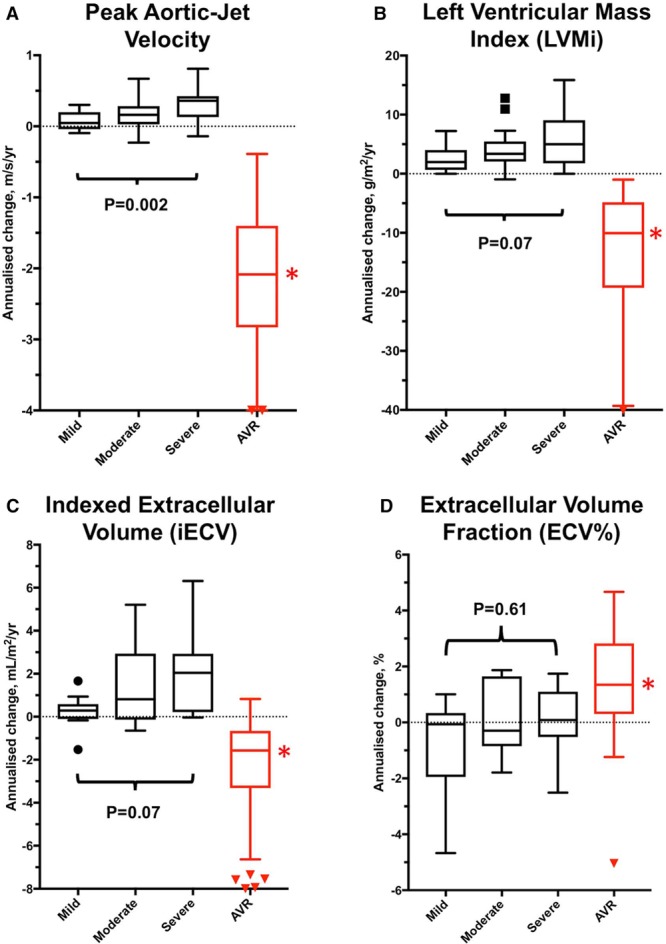
Methods: Asymptomatic and symptomatic patients with aortic stenosis underwent repeat echocardiography and magnetic resonance imaging. Changes in peak aortic-jet velocity, left ventricular mass index, diffuse fibrosis (indexed extracellular volume), and replacement fibrosis (late gadolinium enhancement [LGE]) were quantified.
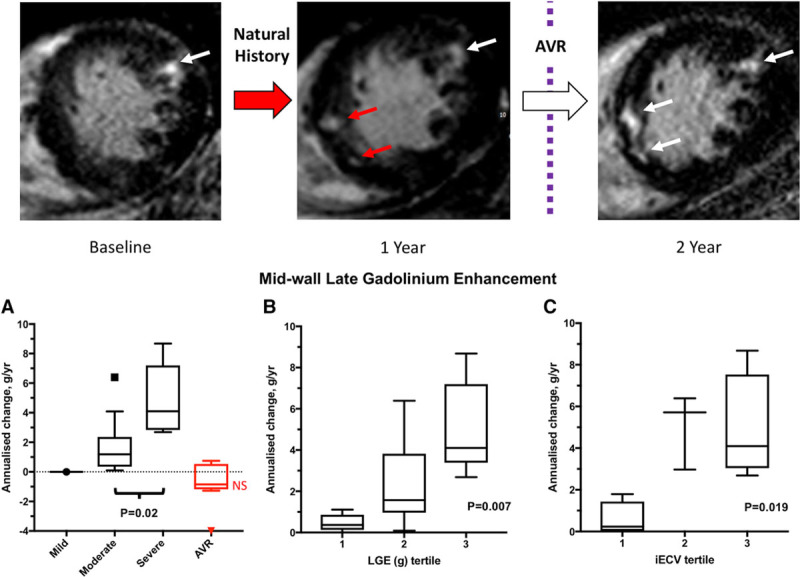
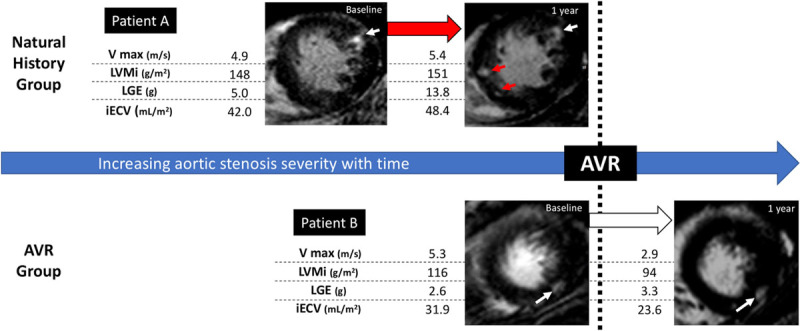
Results: In 61 asymptomatic patients (43% mild, 34% moderate, and 23% severe aortic stenosis), significant increases in peak aortic-jet velocity, left ventricular mass index, indexed extracellular volume, and LGE mass were observed after 2.1±0.7 years, with the most rapid progression observed in patients with most severe stenosis. Patients with baseline midwall LGE (n=16 [26%]; LGE mass, 2.5 g [0.8-4.8 g]) demonstrated particularly rapid increases in scar burden (78% [50%-158%] increase in LGE mass per year). In 38 symptomatic patients (age, 66±8 years; 76% men) who underwent AVR, there was a 19% (11%-25%) reduction in left ventricular mass index (P<0.0001) and an 11% (4%-16%) reduction in indexed extracellular volume (P=0.003) 0.9±0.3 years after surgery. By contrast midwall LGE (n=10 [26%]; mass, 3.3 g [2.6-8.0 g]) did not change post-AVR (n=10; 3.5 g [2.1-8.0 g]; P=0.23), with no evidence of regression even out to 2 years.
Conclusions: In patients with aortic stenosis, cellular hypertrophy and diffuse fibrosis progress in a rapid and balanced manner but are reversible after AVR. Once established, midwall LGE also accumulates rapidly but is irreversible post valve replacement. Given its adverse long-term prognosis, prompt AVR when midwall LGE is first identified may improve clinical outcomes.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifiers: NCT01755936 and NCT01679431.
Keywords: aortic valve stenosis; fibrosis; gadolinium; hypertrophy; magnetic resonance imaging.
© 2018 The Authors.
Figures
Comment in
-
Myocardial Hypertrophy, Matrix Expansion, and Focal Scar: Progression and Regression in Aortic Stenosis.Circ Cardiovasc Imaging. 2018 Jun;11(6):e007975. doi: 10.1161/CIRCIMAGING.118.007975. Circ Cardiovasc Imaging. 2018. PMID: 29914870 No abstract available.
References
-
- Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Bärwolf C, Levang OW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24:1231–1243. - PubMed
-
- Dweck MR, Boon NA, Newby DE. Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol. 2012;60:1854–1863. doi: 10.1016/j.jacc.2012.02.093. - PubMed
-
- Hein S, Arnon E, Kostin S, Schönburg M, Elsässer A, Polyakova V, Bauer EP, Klövekorn WP, Schaper J. Progression from compensated hypertrophy to failure in the pressure-overloaded human heart: structural deterioration and compensatory mechanisms. Circulation. 2003;107:984–991. - PubMed
-
- Dweck MR, Joshi S, Murigu T, Alpendurada F, Jabbour A, Melina G, Banya W, Gulati A, Roussin I, Raza S, Prasad NA, Wage R, Quarto C, Angeloni E, Refice S, Sheppard M, Cook SA, Kilner PJ, Pennell DJ, Newby DE, Mohiaddin RH, Pepper J, Prasad SK. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J Am Coll Cardiol. 2011;58:1271–1279. doi: 10.1016/j.jacc.2011.03.064. - PubMed
-
- Azevedo CF, Nigri M, Higuchi ML, Pomerantzeff PM, Spina GS, Sampaio RO, Tarasoutchi F, Grinberg M, Rochitte CE. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J Am Coll Cardiol. 2010;56:278–287. doi: 10.1016/j.jacc.2009.12.074. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
