

Pharmacokinetics of Tedizolid in Plasma and Sputum of Adults with Cystic Fibrosis
- PMID: 29914949
- PMCID: PMC6125567
- DOI: 10.1128/AAC.00550-18
Pharmacokinetics of Tedizolid in Plasma and Sputum of Adults with Cystic Fibrosis
Abstract
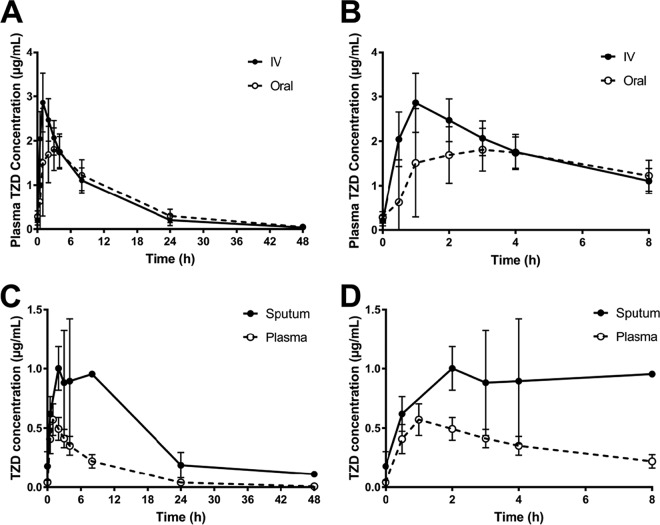
Over the past decade, the prevalence of infections involving methicillin-resistant Staphylococcus aureus (MRSA) in patients with cystic fibrosis (CF) has increased significantly. Tedizolid (TZD) demonstrates excellent activity against MRSA and a favorable safety profile. The pharmacokinetics of several antibiotics have been shown to be altered in CF patients. The purpose of this study was to characterize the pharmacokinetics of tedizolid in this population. Eleven patients with CF were randomized to receive tedizolid phosphate at 200 mg orally or intravenously once daily for 3 doses with a minimum 2-day washout, followed by crossover to the remaining dosage form. Plasma and expectorated sputum were collected following the third dose of each dosage form for analysis. Population pharmacokinetic analysis was performed using the maximum likelihood expectation maximization method, and the disposition of TZD was described by a two-compartment model. The sputum concentrations exceeded the unbound plasma concentrations with an estimated mean sputum-to-unbound plasma penetration ratio of 2.88 (coefficient of variation, 50.3%). The estimated population mean ± standard deviation of total clearance, central volume of distribution, and bioavailability were 9.72 ± 1.62 liters/h, 61.6 ± 6.94 liters, and 1.04 ± 0.232, respectively. The total clearance was higher in CF patients than in healthy volunteers; however, it was similar to published data for patients with complicated skin and skin structure infections (cSSSIs). This study demonstrates that the oral bioavailability of tedizolid is excellent in patients with CF and that the plasma pharmacokinetics are similar to those reported for patients with cSSSIs.
Keywords: cystic fibrosis; pharmacokinetics; tedizolid.
Copyright © 2018 American Society for Microbiology.
Figures


References
-
- Chmiel JF, Aksamit TR, Chotirmall SH, Dasenbrook EC, Elborn JS, LiPuma JJ, Ranganathan SC, Waters VJ, Ratjen FA. 2014. Antibiotic management of lung infections in cystic fibrosis. I. The microbiome, methicillin-resistant Staphylococcus aureus, gram-negative bacteria, and multiple infections. Ann Am Thorac Soc 11:1120–1129. doi:10.1513/AnnalsATS.201402-050AS. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
