

Diabetes Mellitus Secondary to Cushing's Disease
- PMID: 29915558
- PMCID: PMC5994748
- DOI: 10.3389/fendo.2018.00284
Diabetes Mellitus Secondary to Cushing's Disease
Abstract
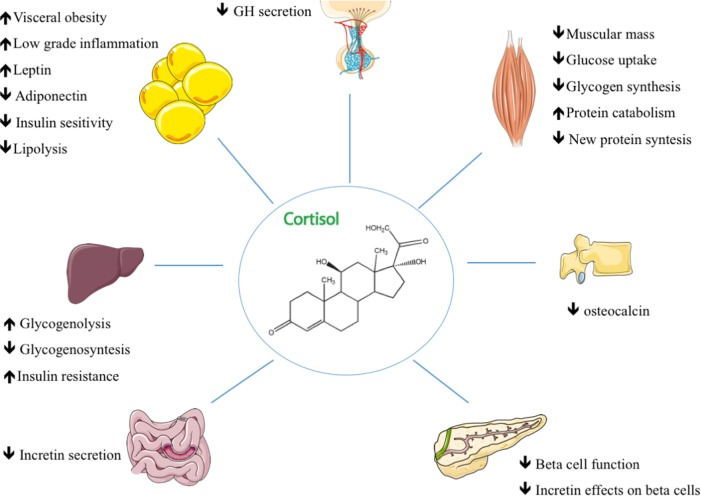
Associated with important comorbidities that significantly reduce patients' overall wellbeing and life expectancy, Cushing's disease (CD) is the most common cause of endogenous hypercortisolism. Glucocorticoid excess can lead to diabetes, and although its prevalence is probably underestimated, up to 50% of patients with CD have varying degrees of altered glucose metabolism. Fasting glycemia may nevertheless be normal in some patients in whom glucocorticoid excess leads primarily to higher postprandial glucose levels. An oral glucose tolerance test should thus be performed in all CD patients to identify glucose metabolism abnormalities. Since diabetes mellitus (DM) is a consequence of cortisol excess, treating CD also serves to alleviate impaired glucose metabolism. Although transsphenoidal pituitary surgery remains the first-line treatment for CD, it is not always effective and other treatment strategies may be necessary. This work examines the main features of DM secondary to CD and focuses on antidiabetic drugs and how cortisol-lowering medication affects glucose metabolism.
Keywords: Cushing’s disease; cortisol-lowering medication; diabetes; glucocorticoids; insulin resistance.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources