

Use of rotational atherectomy for reducing significant dissection in treating de novo femoropopliteal steno-occlusive disease after balloon angioplasty
- PMID: 29915614
- PMCID: PMC5997615
- DOI: 10.11909/j.issn.1671-5411.2018.04.006
Use of rotational atherectomy for reducing significant dissection in treating de novo femoropopliteal steno-occlusive disease after balloon angioplasty
Abstract
Background: Development of arterial dissection is thought to be an important key factor for bailout stenting in femoropopliteal disease. We aimed to evaluate the difference in dissection rate and outcomes between the treatment group with rotational atherectomy and without it.
Methods: From January 2011 to October 2016, we compared the angiography after balloon angioplasty (BA) of de-novo, femoropopliteal, steno-occlusive lesions whether they were treated by rotational atherectomy prior to the BA or not. Fifty-nine lesions (8 occlusions; 3 involving popliteal segment; lesion length: 86.3 ± 66.8 mm) in 44 patients (29 males; mean age 66.9 ± 9.7 years) were enrolled for this review.
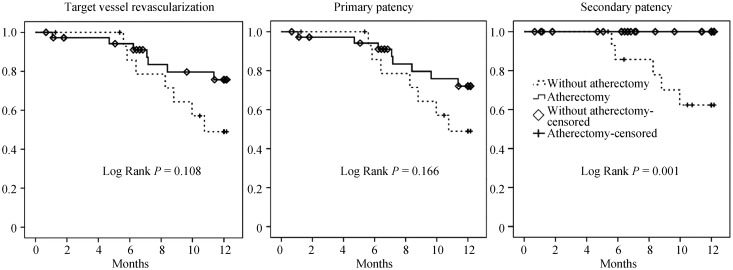
Results: Forty-two lesions were treated using rotational atherectomy, prior to BA while 17 were recanalized firstly by BA. Clinical and lesion characteristics were not different between the groups. However, the rate of significant arterial dissection (type C to F) was lower in the atherectomy group (88.2% vs. 42.9%; P = 0.001). In multivariate analysis, use of the atherectomy device was the only risk factor for prevention of development of significant dissection (P = 0.013; OR = 0.12; 95% CI: 0.025-0.642). Patients were treated either by the angioplasty alone, drug coated balloon or stent insertion. There was lower trend in target vessel revascularization and primary patency toward the atherectomy group (low rank P = 0.108 and 0.166), however secondary patency was significantly better (low rank P = 0.001).
Conclusions: Rotational atherectomy before BA reduced the rate of significant dissection and therefore, might be a valuable option for minimizing need of bailout stenting.
Keywords: Arterial dissection; Atherectomy; Femoropopliteal disease; Peripheral arterial disease.
Figures
References
-
- Laird JR, Katzen BT, Scheinert D, et al. Nitinol stent implantation vs. balloon angioplasty for lesions in the superficial femoral and proximal popliteal arteries of patients with claudication: three-year follow-up from the RESILIENT randomized trial. J Endovasc Ther. 2012;19:1–9. - PubMed
-
- Acin F, de Haro J, Bleda S, Varela C, Esparza L. Primary nitinol stenting in femoropopliteal occlusive disease: a meta-analysis of randomized controlled trials. J Endovasc Ther. 2012;19:585–595. - PubMed
-
- Sabeti S, Schillinger M, Amighi J, et al. Primary patency of femoropopliteal arteries treated with nitinol versus stainless steel self-expanding stents: propensity score-adjusted analysis. Radiology. 2004;232:516–521. - PubMed
-
- Werk M, Albrecht T, Meyer DR, et al. Paclitaxel-coated balloons reduce restenosis after femoro-popliteal angioplasty: evidence from the randomized PACIFIER trial. Circ Cardiovasc Interv. 2012;5:831–840. - PubMed
-
- Foley TR, Cotter RP, Kokkinidis DG, et al. Mid-term outcomes of orbital atherectomy combined with drug-coated balloon angioplasty for treatment of femoropopliteal disease. Catheter Cardiovasc Interv. 2017;89:1078–1085. - PubMed
LinkOut - more resources
Full Text Sources