

Trends and Variation in Oral Anticoagulant Choice in Patients with Atrial Fibrillation, 2010-2017
- PMID: 29920705
- PMCID: PMC6448138
- DOI: 10.1002/phar.2158
Trends and Variation in Oral Anticoagulant Choice in Patients with Atrial Fibrillation, 2010-2017
Abstract
Objective: Since 2010, several non-vitamin K antagonist oral anticoagulants (NOACs) have been brought to the U.S. market, yet little is known regarding their evolving adoption for prophylaxis of atrial fibrillation (AF)-related stroke. We examined temporal trends in choice of oral anticoagulants (OACs) among incident OAC users with AF and its association with patient demographic and clinical characteristics.
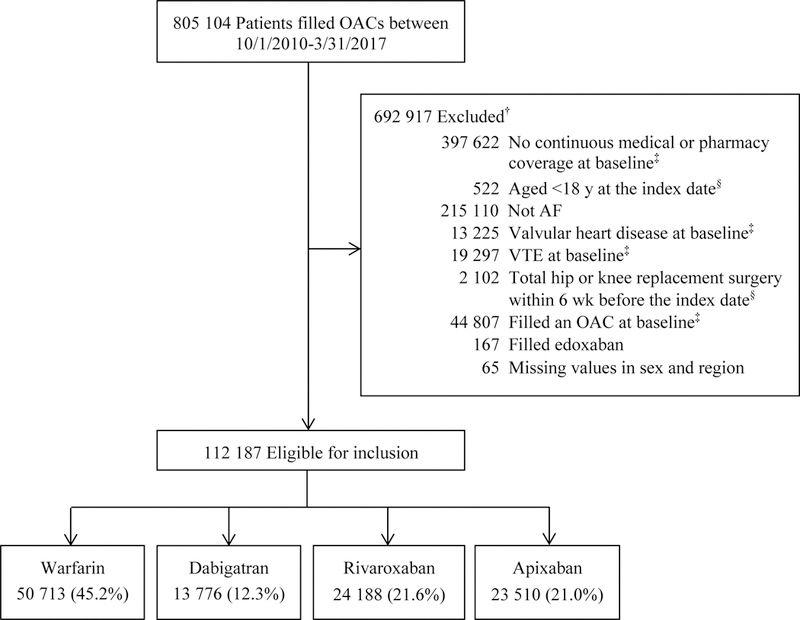
Methods: We conducted a serial cross-sectional analysis of medical and pharmacy claims for commercial and Medicare Advantage enrollees in a large, private, U.S. health plan. We identified 112,187 adults with nonvalvular AF starting OACs between October 2010 and March 2017. Multivariable logistic regression was used to examine the associations of patient characteristics with prescription of NOACs versus warfarin. Multinomial logistic regression was used to test the associations of patient characteristics with choice among NOACs.
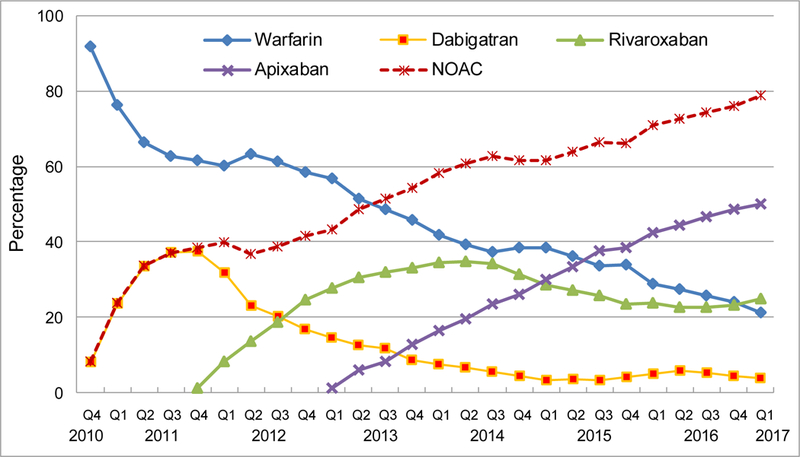
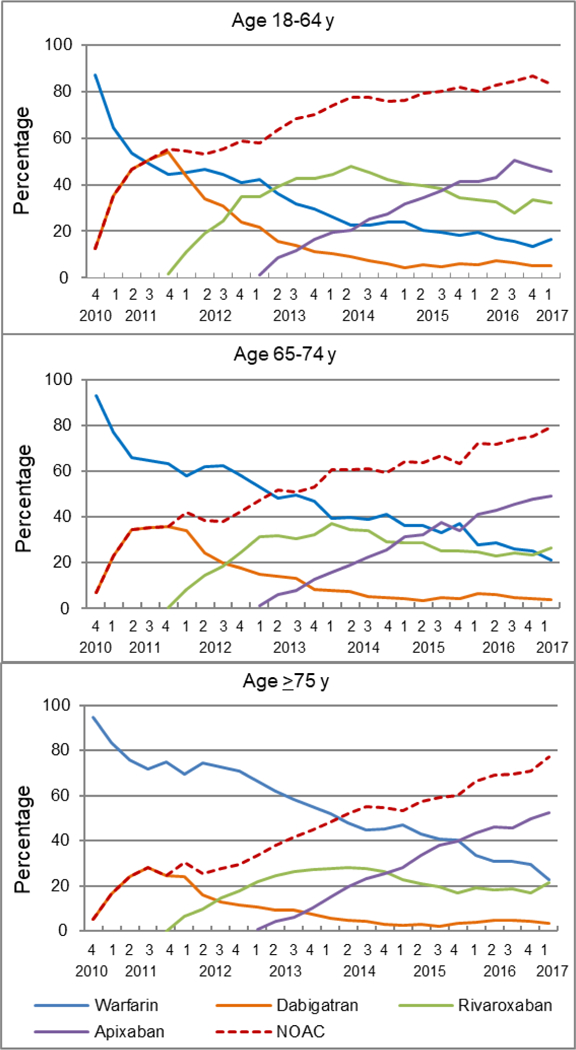
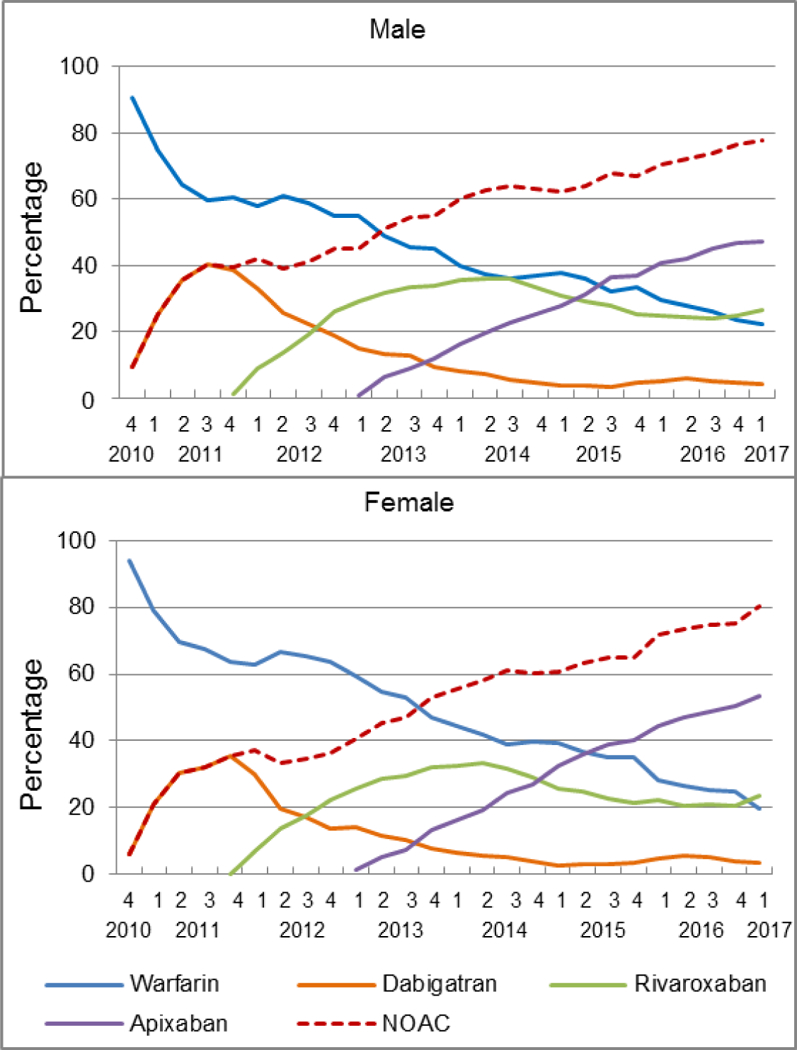
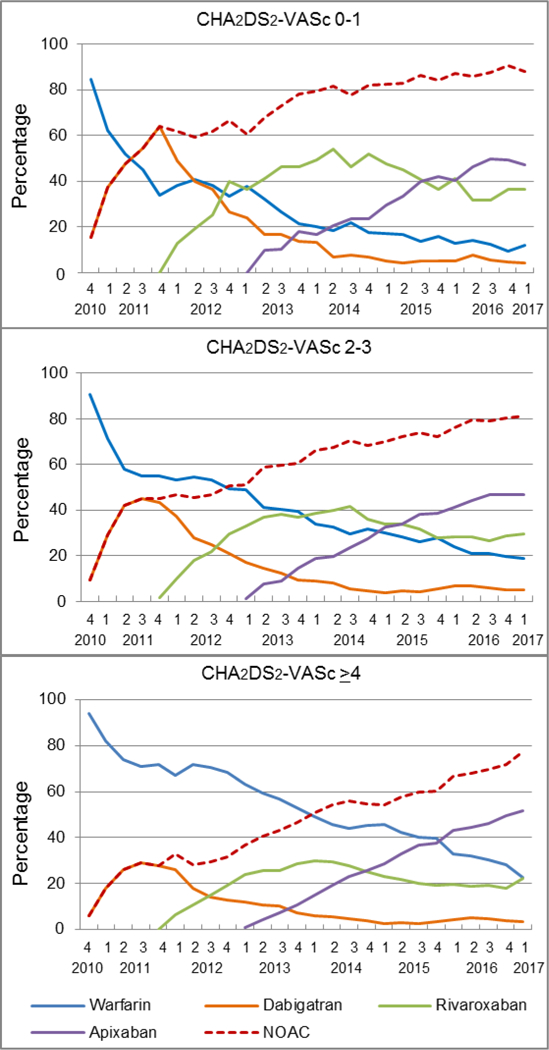
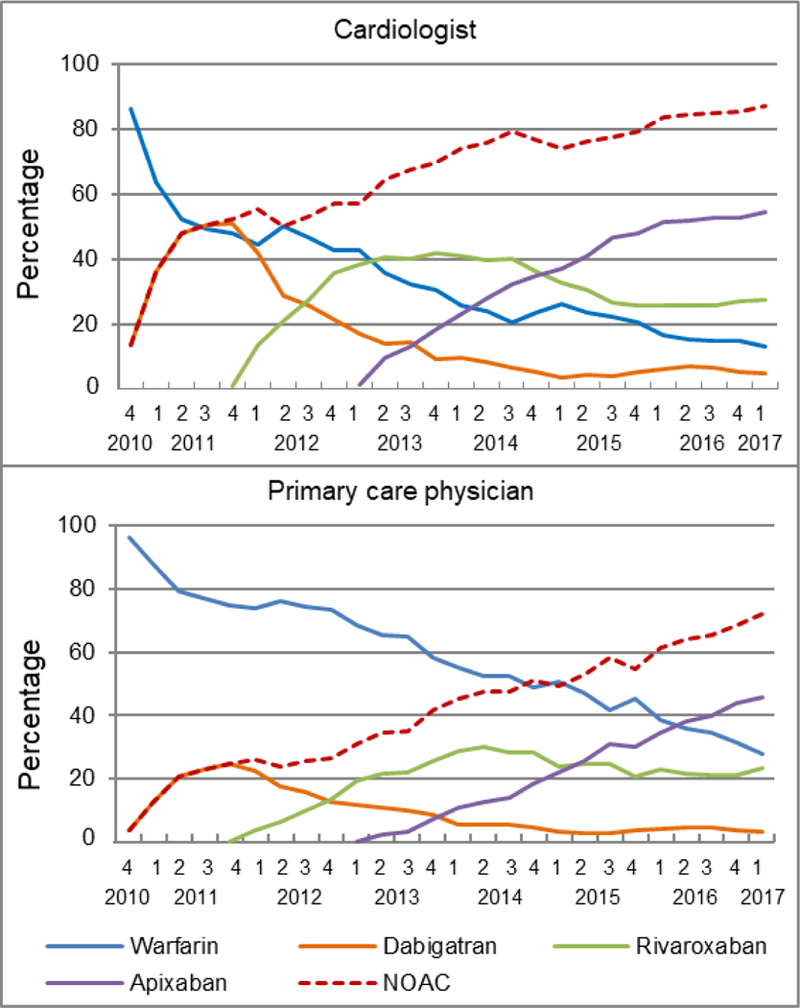
Results: The prescription of NOACs has increased dramatically since their introduction in October 2010. In the first quarter of 2017 (2017Q1), 7502 patients started OACs, of whom 78.9% used NOACs and 21.1% warfarin. For NOACs, 3.8% used dabigatran, 25.0% rivaroxaban, and 50.1% apixaban. In multivariable analyses, factors associated with choice of NOACs versus warfarin included younger age, lower stroke or bleeding risk, fewer comorbidities, higher education level or household net worth, and prescription by cardiologists (all p<0.001). There was no sex difference in likelihood of filling NOACs versus warfarin in 2010Q4-2012, but women had higher odds of starting NOACs (odds ratio = 1.19; 95% confidence interval = 1.14-1.25) in 2015-2017Q1. Among NOAC users, the odds of apixaban prescription increased with age, female sex, stroke or bleeding risk, and comorbidities (all p<0.05).
Conclusion: NOAC prescriptions have increased substantially among incident OAC users with nonvalvular AF, predominantly driven by increased prescription of apixaban. Warfarin and apixaban were generally preferred for elderly patients, patients with higher stroke or bleeding risk, and patients with more comorbidities.
Keywords: atrial fibrillation; choice; oral anticoagulant; temporal trend.
© 2018 Pharmacotherapy Publications, Inc.
Conflict of interest statement
Conflict of interest statement
Dr. Alexander is Chair of FDA’s Peripheral and Central Nervous System Advisory Committee, serves as a paid advisor to QuintilesIMS, serves on the advisory board of MesaRx Innovations, is a member of OptumRx’s National P&T Committee; and holds equity in Monument Analytics. Dr. Nazarian is a consultant to Biosense Webster, Siemens, St Jude Medical, and CardioSolv and receives research grants from Biosense Webster, Siemens, and Imricor. These arrangements have been reviewed and approved by Johns Hopkins University and the University of Pennsylvania, in accordance with respective conflict of interest policies.
Figures
References
-
- Lip GY, Lane DA. Stroke prevention in atrial fibrillation: a systematic review. JAMA 2015;313:1950–1962. - PubMed
-
- Hylek EM, Go AS, Chang Y, et al. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med 2003;349:1019–1026. - PubMed
-
- Moss JD, Cifu AS. Management of anticoagulation in patients with atrial fibrillation. JAMA 2015;314:291–292. - PubMed
-
- Mega JL. A new era for anticoagulation in atrial fibrillation. N Engl J Med 2011;365:1052–1054. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–1151. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
