

An expert consensus to standardise definitions, diagnosis and treatment targets for anti-fibrotic stricture therapies in Crohn's disease
- PMID: 29920726
- PMCID: PMC6043370
- DOI: 10.1111/apt.14853
An expert consensus to standardise definitions, diagnosis and treatment targets for anti-fibrotic stricture therapies in Crohn's disease
Abstract
Background: Fibrotic stricture is a common complication of Crohn's disease (CD) affecting approximately half of all patients. No specific anti-fibrotic therapies are available; however, several therapies are currently under evaluation. Drug development for the indication of stricturing CD is hampered by a lack of standardised definitions, diagnostic modalities, clinical trial eligibility criteria, endpoints and treatment targets in stricturing CD.
Aim: To standardise definitions, diagnosis and treatment targets for anti-fibrotic stricture therapies in Chron's disease.
Methods: An interdisciplinary expert panel consisting of 15 gastroenterologists and radiologists was assembled. Using modified RAND/University of California Los Angeles appropriateness methodology, 109 candidate items derived from systematic review and expert opinion focusing on small intestinal strictures were anonymously rated as inappropriate, uncertain or appropriate. Survey results were discussed as a group before a second and third round of voting.
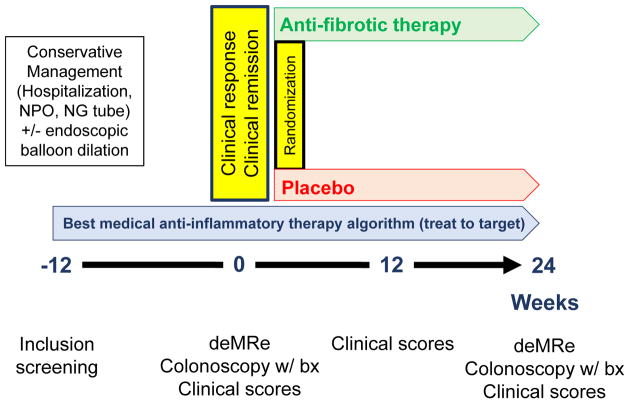
Results: Fibrotic strictures are defined by the combination of luminal narrowing, wall thickening and pre-stenotic dilation. Definitions of anastomotic (at site of prior intestinal resection with anastomosis) and naïve small bowel strictures were similar; however, there was uncertainty regarding wall thickness in anastomotic strictures. Magnetic resonance imaging is considered the optimal technique to define fibrotic strictures and assess response to therapy. Symptomatic strictures are defined by abdominal distension, cramping, dietary restrictions, nausea, vomiting, abdominal pain and post-prandial abdominal pain. Need for intervention (endoscopic balloon dilation or surgery) within 24-48 weeks is considered the appropriate endpoint in pharmacological trials.
Conclusions: Consensus criteria for diagnosis and response to therapy in stricturing Crohn's disease should inform both clinical practice and trial design.
© 2018 John Wiley & Sons Ltd.
Figures
Comment in
-
Editorial: treating strictures in inflammatory bowel disease.Aliment Pharmacol Ther. 2018 Dec;48(11-12):1312-1313. doi: 10.1111/apt.14987. Aliment Pharmacol Ther. 2018. PMID: 30488631 No abstract available.
References
-
- Oberhuber G, Stangl PC, Vogelsang H, et al. Significant association of strictures and internal fistula formation in Crohn’s disease. Virchows Arch. 2000;437:293–297. - PubMed
-
- Orscheln ES, Dillman JR, Towbin AJ, et al. Penetrating Crohn disease: does it occur in the absence of stricturing disease? Abdom Radiol (NY) 2017 e-pub ahead of print. - PubMed
-
- Jairath V, Levesque BG, Vande Casteele N, et al. Evolving concepts in phases I and II drug development for Crohn’s disease. J Crohns Colitis. 2017;11:246–255. - PubMed
-
- Neurath MF. Current and emerging therapeutic targets for IBD. Nat Rev Gastroenterol Hepatol. 2017;14:269–278. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical