

Physical fitness interventions for nonambulatory stroke survivors: A mixed-methods systematic review and meta-analysis
- PMID: 29920979
- PMCID: PMC6043697
- DOI: 10.1002/brb3.1000
Physical fitness interventions for nonambulatory stroke survivors: A mixed-methods systematic review and meta-analysis
Abstract
Introduction: Physical fitness training after stroke is recommended in guidelines across the world, but evidence pertains mainly to ambulatory stroke survivors. Nonambulatory stroke survivors (FAC score ≤2) are at increased risk of recurrent stroke due to limited physical activity. This systematic review aimed to synthesize evidence regarding case fatality, effects, experiences, and feasibility of fitness training for nonambulatory stroke survivors.
Methods: Eight major databases were searched for any type of study design. Two independent reviewers selected studies, extracted data, and assessed study quality, using published tools. Random-effects meta-analysis was used. Following their separate analysis, qualitative and quantitative data were synthesized using a published framework.
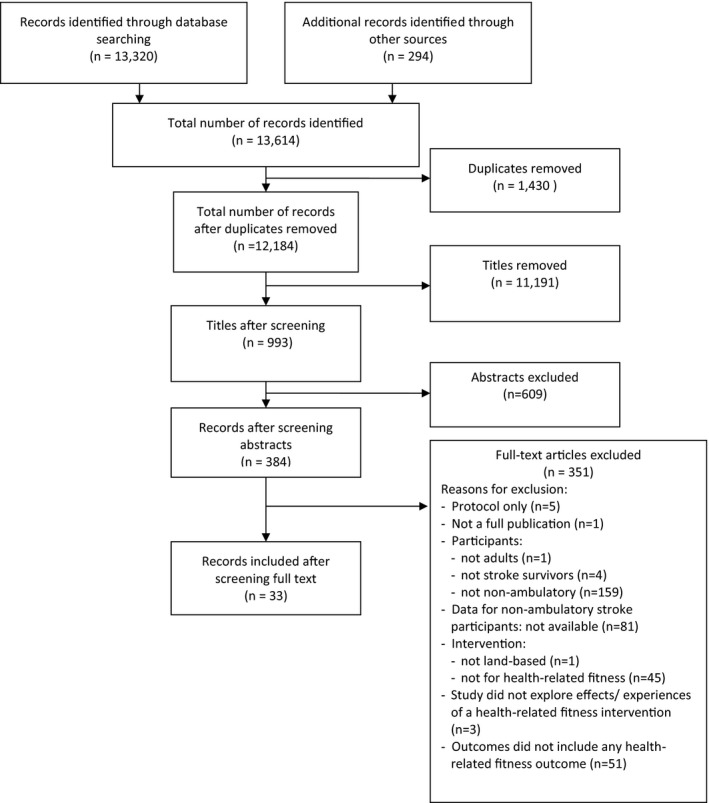
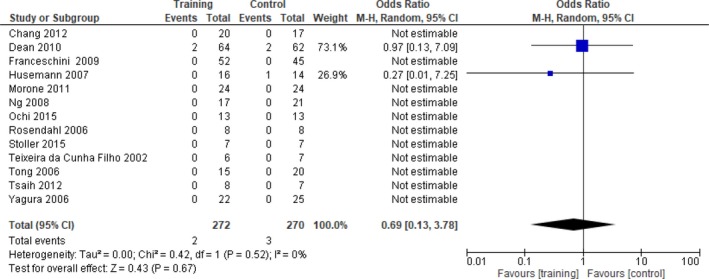
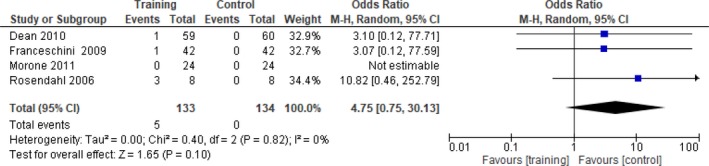
Results: Of 13,614 records, 33 studies involving 910 nonambulatory participants met inclusion criteria. Most studies were of moderate quality. Interventions comprised assisted walking (25 studies), cycle ergometer training (5 studies), and other training (3 studies), mainly in acute settings. Case fatality did not differ between intervention (1.75%) and control (0.88%) groups (95% CI 0.13-3.78, p = 0.67). Compared with control interventions, assisted walking significantly improved: fat mass, peak heart rate, peak oxygen uptake and walking endurance, maximum walking speed, and mobility at intervention end, and walking endurance, balance, mobility, and independent walking at follow-up. Cycle ergometry significantly improved peak heart rate, work load, peak ventilation, peak carbon dioxide production, HDL cholesterol, fasting insulin and fasting glucose, and independence at intervention end. Effectiveness of other training could not be established. There were insufficient qualitative data to draw conclusions about participants' experiences, but those reported were positive. There were few intervention-related adverse events, and dropout rate ranged from 12 to 20%.
Conclusions: Findings suggest safety, effectiveness, and feasibility of adapted fitness training for screened nonambulatory stroke survivors. Further research needs to investigate the clinical and cost-effectiveness as well as experiences of fitness training-especially for chronic stroke survivors in community settings.
Keywords: exercise; fitness; nonambulatory; rehabilitation; stroke; systematic review.
© 2018 The Authors. Brain and Behavior published by Wiley Periodicals, Inc.
Figures










References
-
- American Association for Clinical Chemistry (2017a). Lab tests online: Lipid profiles. Retrieved from https://labtestsonline.org/understanding/analytes/lipid/tab/test/. Updated September 15, 2017. [Accessed November 23].
-
- American Association for Clinical Chemistry (2017b). Lab tests online: Glucose tests. Retrieved from https://labtestsonline.org/understanding/analytes/glucose/tab/test/. Updated January 16, 2017. [Accessed November 23, 2017].
-
- American College of Sports Medicine (2013). ACSM's guidelines for exercise testing and prescription. Philadelphia, PA: Lippincott Williams & Wilkins. - PubMed
-
- Armijo‐Olivo, S. , Stiles, C. R. , Hagen, N. A. , Biondo, P. D. , & Cummings, G. G. (2012). Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. Journal of Evaluation in Clinical Practice, 18(1), 12–18. 10.1111/j.1365-2753.2010.01516.x - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
