

Patient-reported outcomes from a randomized phase III trial of sarilumab monotherapy versus adalimumab monotherapy in patients with rheumatoid arthritis
- PMID: 29921318
- PMCID: PMC6009058
- DOI: 10.1186/s13075-018-1614-z
Patient-reported outcomes from a randomized phase III trial of sarilumab monotherapy versus adalimumab monotherapy in patients with rheumatoid arthritis
Abstract
Background: The phase III MONARCH randomized controlled trial (NCT02332590) demonstrated that in patients with rheumatoid arthritis (RA), sarilumab (anti-interleukin-6 receptor monoclonal antibody) monotherapy is superior to adalimumab monotherapy in reducing disease activity and signs and symptoms of RA, as well as in improving physical function, with similar rates of adverse and serious adverse events. We report the effects of sarilumab versus adalimumab on patient-reported outcomes (PROs).
Methods: Patients with active RA intolerant of, or inadequate responders to, methotrexate were randomized to sarilumab 200 mg plus placebo every 2 weeks (q2w; n = 184) or adalimumab 40 mg plus placebo q2w (n = 185). Dose escalation to weekly administration of adalimumab or matching placebo was permitted at week 16. PROs assessed at baseline and weeks 12 and 24 included patient global assessment of disease activity (PtGA), pain and morning stiffness visual analogue scales (VASs), Health Assessment Questionnaire Disability Index (HAQ-DI), 36-item Short Form Health Survey (SF-36), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), Rheumatoid Arthritis Impact of Disease (RAID), and rheumatoid arthritis-specific Work Productivity Survey (WPS-RA). Between-group differences in least-squares mean (LSM) changes from baseline were analyzed. p < 0.05 was considered significant for PROs in a predefined hierarchy. For PROs not in the hierarchy, nominal p values are provided. Proportions of patients reporting improvements greater than or equal to the minimal clinically important difference (MCID) and achieving normative values were assessed.
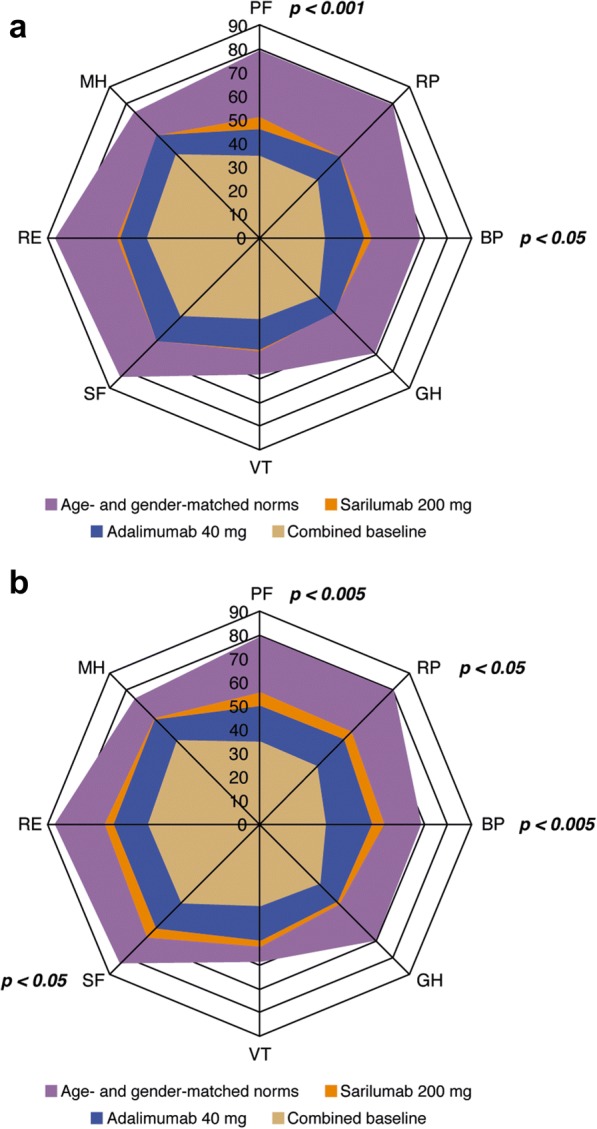
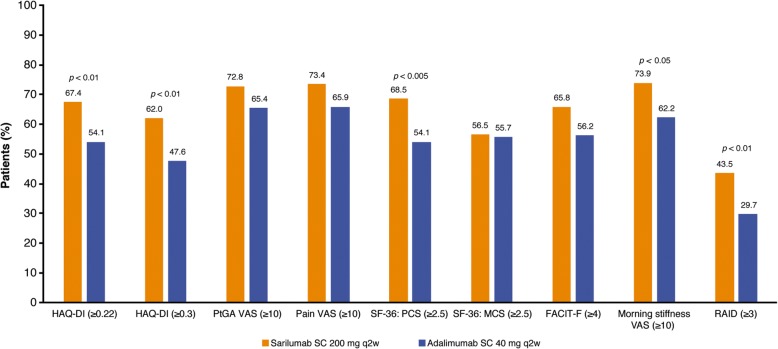
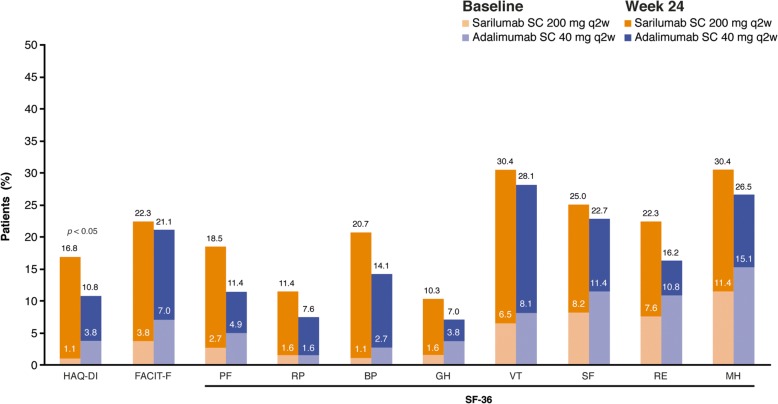
Results: At week 24, sarilumab treatment resulted in significantly greater LSM changes from baseline than adalimumab monotherapy in HAQ-DI (p < 0.005), PtGA (p < 0.001), pain VAS (p < 0.001), and SF-36 Physical Component Summary (PCS) (p < 0.001). Greater LSM changes were reported for sarilumab than for adalimumab in RAID (nominal p < 0.001), morning stiffness VAS (nominal p < 0.05), and WPS-RA (nominal p < 0.005). Between-group differences in FACIT-F and SF-36 Mental Component Summary (MCS) were not significant. More patients reported improvements greater than or equal to the MCID in HAQ-DI (nominal p < 0.01), RAID (nominal p < 0.01), SF-36 PCS (nominal p < 0.005), and morning stiffness (nominal p < 0.05), as well as greater than or equal to the normative values in HAQ-DI (p < 0.05), with sarilumab versus adalimumab.
Conclusions: In parallel with the clinical efficacy profile previously reported, sarilumab monotherapy resulted in greater improvements across multiple PROs than adalimumab monotherapy.
Trial registration: ClinicalTrials.gov, NCT02332590 . Registered on 5 January 2015.
Keywords: Adalimumab; Biologic disease-modifying antirheumatic drugs; Patient-reported outcomes; Rheumatoid arthritis; Sarilumab.
Conflict of interest statement
Ethics approval and consent to participate
The protocol received approval from the institutional review board and independent ethics committee of the investigational centers and was performed in accordance with the Declaration of Helsinki. All patients provided written consent prior to study participation, and the trial was conducted in compliance with institutional review board regulations, the International Conference on Harmonisation Guidelines for Good Clinical Practice, and the Declaration of Helsinki. The specific ethical bodies that approved study are as follows: Comité de Ética Científico, S.S.M. Oriente, Chile; Eticka komise, Revmatologickeho ustavu, Czech Republic; EK FN Královské, Vinohrady, FN Kralovske Vinohrady, Czech Republic; Eticka komise, Uherskohradistske nemocnice, a.s., Czech Republic; Ethik-Kommission des Landes Berlin, Landesamt für Gesundheit und Soziales, Berlin, Germany; Medical Research Council, Ethics Committee for Clinical Pharmacology, Hungary; Ethics Committee of Tel Aviv, Sourasky Medical Center, Israel; EC of Sheba Medical Center, The Chaim Sheba Medical Center, Israel; Ethics Committee of Carmel Medical Center, Israel; Seoul National University Hospital, Republic of Korea; Eulji University Hospital, Republic of Korea; Keimyung University, Dongsan Medical Center, Republic of Korea; CE de la asociación benéfica Prisma Carlos Gonzales, Peru; Komisja Bioetyczna przy Okregowej Radzie Lekarskiej WIL, Poland; National Bioethics Committee of Medical Product and Medical Devices, Romania; LEC of the Scientific Research Institute of Rheumatology, Russian Federation; Ethics Board at Ministry of Health of the Russian Federation, Russian Federation; LEC of the Kemerovo State Medical Academy, Russian Federation; LEC of the Saintpetersburg I.I. Dzhanelidze Research Institute, Russian Federation; LEC of Saratov Regional Clinical Hospital, Russian Federation; LEC of ‘Applied Medicine’, Russian Federation; LEC of the Moscow City Hospital n.a. S. P. Botkin, Russian Federation; LEC of the City Clinical Hospital n.a. M.E. Zhadkevich, Russian Federation; Pharma Ethics (Pty) Ltd., South Africa; CEIC Corporació Sanitària del Parc Taulí, Spain; LEC of the Regional Clinical Hospital n.a. N.I. Pyrogov, Ukraine; LEC of Consultative Diagnostic Center of Pechersky District, Ukraine; LEC of the Ivano-Frankivsk Regional Clinical Hospital, Ukraine; LEC of Lutsk Regional Hospital, Ukraine; LEC of Vinnytsya City Clinical Hospital #1, Ukraine; LEC of Lviv Regional Clinical Diagnostic Center, Ukraine; LEC Kyiv City Clinical Hospital #3, Ukraine; LEC of MIHC Regional Clinical Hospital, Ukraine; LEC of Poltava Regional Clinical Hospital n.a. Sklyfosofsky, Ukraine; NRES Committee London – London Bridge National Research Ethics Service, United Kingdom; Chesapeake IRB, United States; Comité de Protection des Personnes Est III Hôpital de Brabois, France; Ethics Committee of Bnei Zion Medical Center Bnei Zion, Israel; Ethics Committee of Rambam Medical Center, Israel; Ajou University Hospital, Republic of Korea; Chungnam National University Hospital, Republic of Korea; Chosun University Hospital, Republic of Korea; Dong-A University Hospital, Republic of Korea; Wits Human Research EC, South Africa; Dartmouth Medical School IRB, United States.
Competing interests
VS is a consultant for AbbVie, Amgen, AstraZeneca, BMS, Boehringer Ingelheim, Celltrion, Corrona, Crescendo, Genentech/Roche, GSK, Janssen, Eli Lilly & Co., Merck, Novartis, Pfizer, Regeneron, Samsung, Sandoz, Sanofi, and UCB. LG is a member of an institution that received research funding for the present study; a consultant for AbbVie, BMS, Genentech/Roche, Janssen, Eli Lilly & Co., Novartis, Pfizer, and UCB; and a member of the executive committee of the Outcome Measures in Rheumatology initiative. GRB is a member of an institution that received research funding from Sanofi and Regeneron Pharmaceuticals, Inc., for the present study. CWJP, SG, YL, HvH, and MR are employees of and shareholders in Sanofi. TK, CIC, and JvA are employees of and shareholders in Regeneron Pharmaceuticals, Inc. EKM is a shareholder of Pfizer Inc., and Regeneron Pharmaceuticals, Inc., and an employee of Regeneron Pharmaceuticals, Inc.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
