

High prevalence of epilepsy in two rural onchocerciasis endemic villages in the Mahenge area, Tanzania, after 20 years of community directed treatment with ivermectin
- PMID: 29921319
- PMCID: PMC6009039
- DOI: 10.1186/s40249-018-0450-3
High prevalence of epilepsy in two rural onchocerciasis endemic villages in the Mahenge area, Tanzania, after 20 years of community directed treatment with ivermectin
Abstract
Background: Epilepsy is a neurological disorder with a multitude of underlying causes, which may include infection with Onchocerca volvulus, the parasitic worm that causes human onchocerciasis. A survey carried out in 1989 revealed a high prevalence of epilepsy (1.02% overall, ranging from 0.51 to 3.71% in ten villages) in the Mahenge area of Ulanga district, an onchocerciasis endemic region in south eastern Tanzania. This study aimed to determine the prevalence and incidence of epilepsy following 20 years of onchocerciasis control through annual community directed treatment with ivermectin (CDTI).
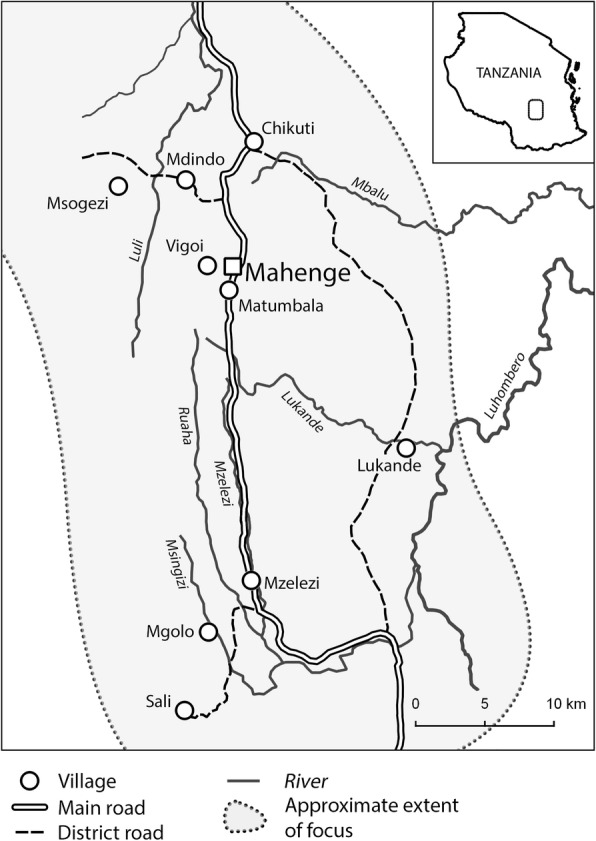
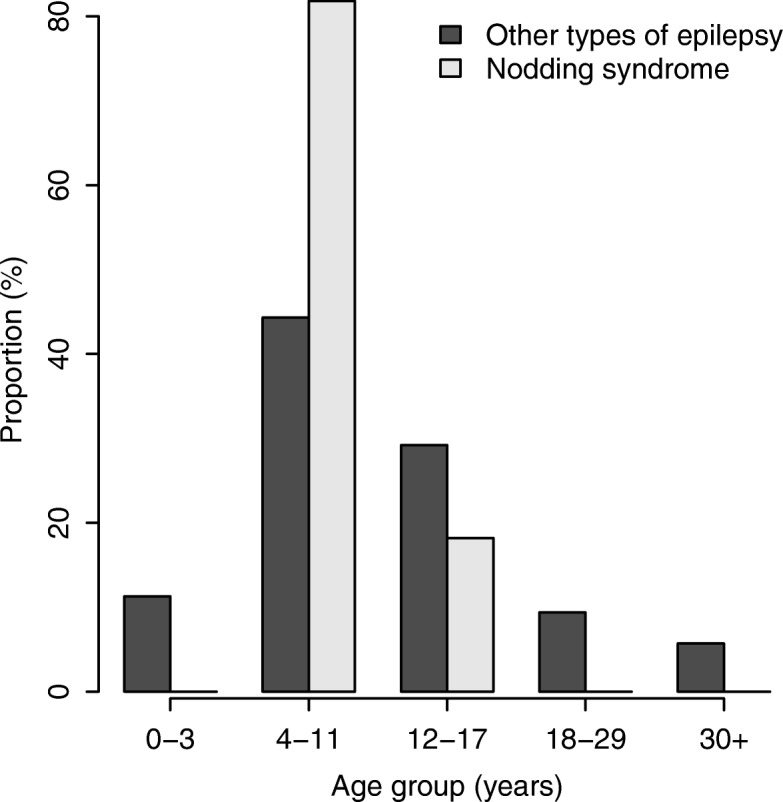
Methods: The study was conducted in January 2017 in two suburban and two rural villages in the Mahenge area. Door-to-door household visits were carried out by trained community health workers and data assistants to screen for persons suspected of having epilepsy, using a standardised questionnaire. Persons with suspected epilepsy were then interviewed and examined by a neurologist for case verification. Onchocerciasis associated epilepsy was defined as epilepsy without an obvious cause, with an onset of seizures between the ages of 3-18 years in previously healthy children. In each village, fifty males aged ≥20 years were tested for onchocerciasis antibodies using an OV16 rapid test and were examined for presence of onchocerciasis nodules. Children aged 6-10 years were also tested using OV16 tests.
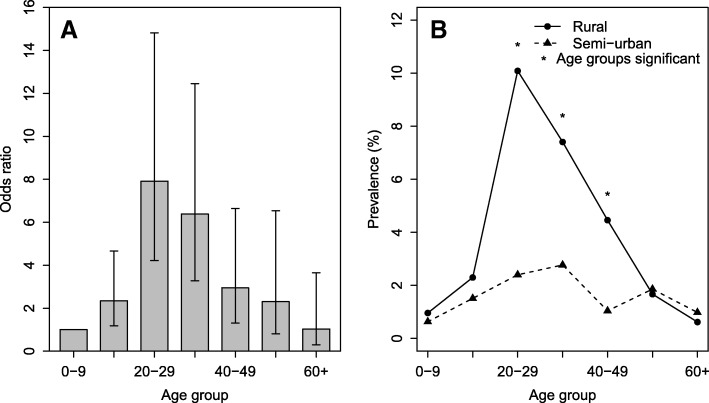
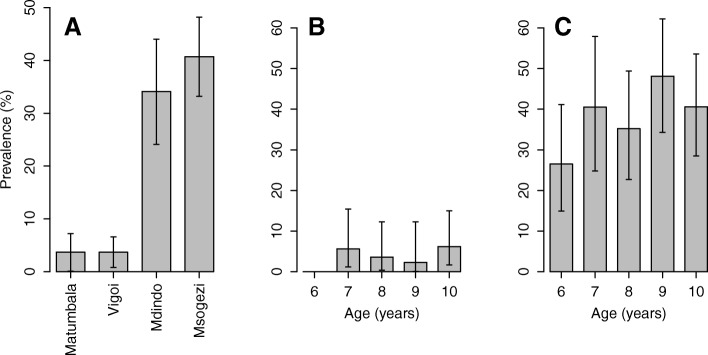
Results: 5117 individuals (median age 18.5 years, 53.2% female) from 1168 households were screened. 244 (4.8%) were suspected of having epilepsy and invited for neurological assessment. Prevalence of epilepsy was 2.5%, with the rural villages having the highest rate (3.5% vs 1.5%), P < 0.001. Overall incidence of epilepsy was 111 cases (95% CI: 73-161) per 100 000 person-years, while that of onchocerciasis associated epilepsy was 131 (95% CI: 70-223). Prevalence of OV16 antibodies in adult males and among children 6-10 years old was higher in rural villages than in suburban villages (76.5% vs 50.6, and 42.6% vs 4.7% respectively), (P < 0.001), while overall prevalence of onchocerciasis nodules was 1.8%.
Conclusions: This survey revealed a high prevalence and incidence of epilepsy in two rural onchocerciasis endemic villages in the Mahenge area. Despite 20 years of CDTI, a high prevalence of OV16 antibodies in children aged 6-10 years suggests on-going O. volvulus transmission. Reasons for the persistence of on-going parasite transmission in the Mahenge area need to be investigated.
Keywords: Epilepsy; Mahenge; Onchocerciasis; Tanzania.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the ethical committees of the National Institute for Medical Research in Tanzania and the University of Antwerp in Belgium. The study was carried out adhering to the principles of the Declaration of Helsinki. Meetings were held with the community leaders to explain the aims and procedures of the study. During the screening phase, consent was obtained from heads of households or adults who were available at the household during the interviews. For persons suspected to have epilepsy and individuals who participated in REMO and in OV16 testing, individual written consent was obtained. Individuals aged 18 years and above provided their own consent, while children and minors had their consent signed by their parents or guardians. Moreover, assent was obtained from those aged 12 years or above.
Competing interests
The authors declare that they have no competing interests.
Figures
Comment in
-
Onchocerciasis-associated epilepsy: another piece in the puzzle from the Mahenge mountains, southern Tanzania.Infect Dis Poverty. 2019 May 24;8(1):35. doi: 10.1186/s40249-019-0545-5. Infect Dis Poverty. 2019. PMID: 31122275 Free PMC article.
References
-
- World Health Organisation. Epilepsy 2017. http://www.who.int/mediacentre/factsheets/fs999/en/. Accessed 28 Sep 2017.
-
- Aall-Jilek LM. Epilepsy in the Wapogoro tribe in Tanganyika. Acta Psychiatr Scand. 1965;41:57–86. doi: 10.1111/j.1600-0447.1965.tb04970.x. - DOI
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
