

Comparison of prostatic artery embolisation (PAE) versus transurethral resection of the prostate (TURP) for benign prostatic hyperplasia: randomised, open label, non-inferiority trial
- PMID: 29921613
- PMCID: PMC6006990
- DOI: 10.1136/bmj.k2338
Comparison of prostatic artery embolisation (PAE) versus transurethral resection of the prostate (TURP) for benign prostatic hyperplasia: randomised, open label, non-inferiority trial
Abstract
Objective: To compare prostatic artery embolisation (PAE) with transurethral resection of the prostate (TURP) in the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia in terms of patient reported and functional outcomes.
Design: Randomised, open label, non-inferiority trial.
Setting: Urology and radiology departments of a Swiss tertiary care centre.
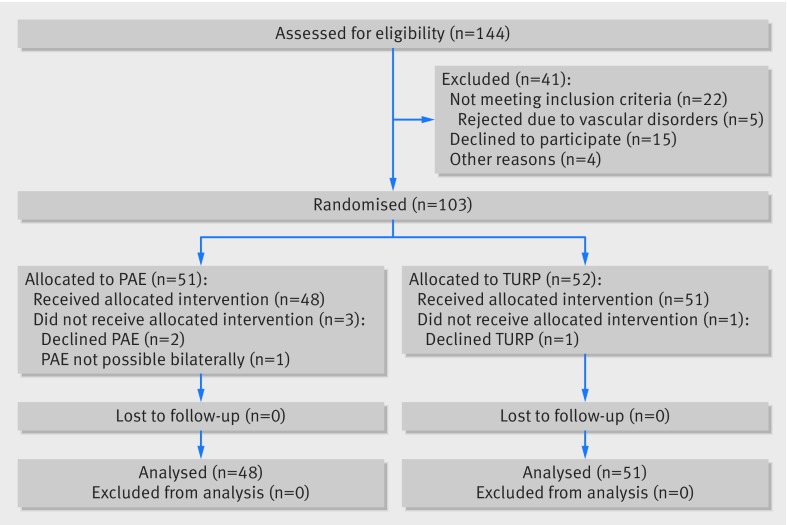
Participants: 103 patients aged ≥40 years with refractory lower urinary tract symptoms secondary to benign prostatic hyperplasia were randomised between 11 February 2014 and 24 May 2017; 48 and 51 patients reached the primary endpoint 12 weeks after PAE and TURP, respectively.
Interventions: PAE performed with 250-400 μm microspheres under local anaesthesia versus monopolar TURP performed under spinal or general anaesthesia.
Main outcomes and measures: Primary outcome was change in international prostate symptoms score (IPSS) from baseline to 12 weeks after surgery; a difference of less than 3 points between treatments was defined as non-inferiority for PAE and tested with a one sided t test. Secondary outcomes included further questionnaires, functional measures, magnetic resonance imaging findings, and adverse events; changes from baseline to 12 weeks were compared between treatments with two sided tests for superiority.
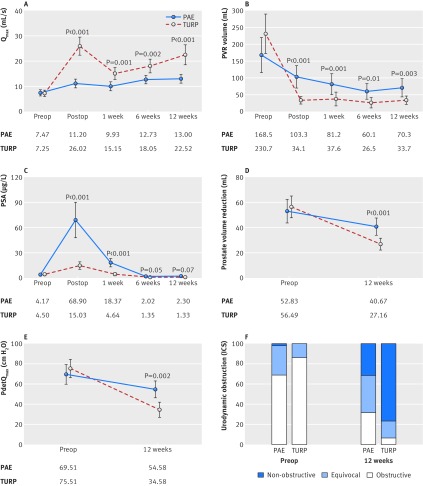
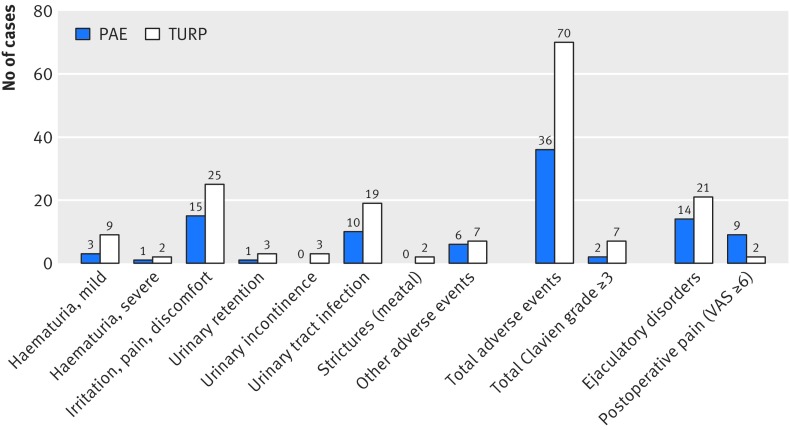
Results: Mean reduction in IPSS from baseline to 12 weeks was -9.23 points after PAE and -10.77 points after TURP. Although the difference was less than 3 points (1.54 points in favour of TURP (95% confidence interval -1.45 to 4.52)), non-inferiority of PAE could not be shown (P=0.17). None of the patient reported secondary outcomes differed significantly between treatments when tested for superiority; IPSS also did not differ significantly (P=0.31). At 12 weeks, PAE was less effective than TURP regarding changes in maximum rate of urinary flow (5.19 v 15.34 mL/s; difference 10.15 (95% confidence interval -14.67 to -5.63); P<0.001), postvoid residual urine (-86.36 v -199.98 mL; 113.62 (39.25 to 187.98); P=0.003), prostate volume (-12.17 v -30.27 mL; 18.11 (10.11 to 26.10); P<0.001), and desobstructive effectiveness according to pressure flow studies (56% v 93% shift towards less obstructive category; P=0.003). Fewer adverse events occurred after PAE than after TURP (36 v 70 events; P=0.003).
Conclusions: The improvement in lower urinary tract symptoms secondary to benign prostatic hyperplasia seen 12 weeks after PAE is close to that after TURP. PAE is associated with fewer complications than TURP but has disadvantages regarding functional outcomes, which should be considered when selecting patients. Further comparative study findings, including longer follow-up, should be evaluated before PAE can be considered as a routine treatment.
Trial registration: Clinicaltrials.gov NCT02054013.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from St Gallen Cantonal Hospital for the submitted work; no financial relationship with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures

Comment in
-
Re: Comparison of Prostatic Artery Embolization (PAE) Versus Transurethral Resection of the Prostate (TURP) for Benign Prostatic Hyperplasia: Randomised, Open Label, Non-inferiority Trial.Eur Urol. 2018 Dec;74(6):844. doi: 10.1016/j.eururo.2018.07.020. Epub 2018 Aug 3. Eur Urol. 2018. PMID: 30082149 No abstract available.
-
Studie vergleicht Prostata-Embolisation und -Resektion.Aktuelle Urol. 2018 Sep;49(5):387-388. doi: 10.1055/a-0677-9413. Epub 2018 Sep 5. Aktuelle Urol. 2018. PMID: 30184590 German. No abstract available.
References
-
- van Exel NJ, Koopmanschap MA, McDonnell J, Chapple CR, Berges R, Rutten FF, TRIUMPH Pan-European Expert Panel Medical consumption and costs during a one-year follow-up of patients with LUTS suggestive of BPH in six european countries: report of the TRIUMPH study. Eur Urol 2006;49:92-102. 10.1016/j.eururo.2005.09.016. - DOI - PubMed
-
- Gravas S, Cornu JN, Drake MJ, et al. EAU Guidelines on management of non-neurogenic male lower urinary tract symptoms (LUTS), incl. benign prostatic obstruction (BPO). 2018 https://uroweb.org/guideline/treatment-of-non-neurogenic-male-luts/.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical