

Validation of discharge diagnosis codes to identify serious infections among middle age and older adults
- PMID: 29921683
- PMCID: PMC6009457
- DOI: 10.1136/bmjopen-2017-020857
Validation of discharge diagnosis codes to identify serious infections among middle age and older adults
Abstract
Objectives: Hospitalisations for serious infections are common among middle age and older adults and frequently used as study outcomes. Yet, few studies have evaluated the performance of diagnosis codes to identify serious infections in this population. We sought to determine the positive predictive value (PPV) of diagnosis codes for identifying hospitalisations due to serious infections among middle age and older adults.
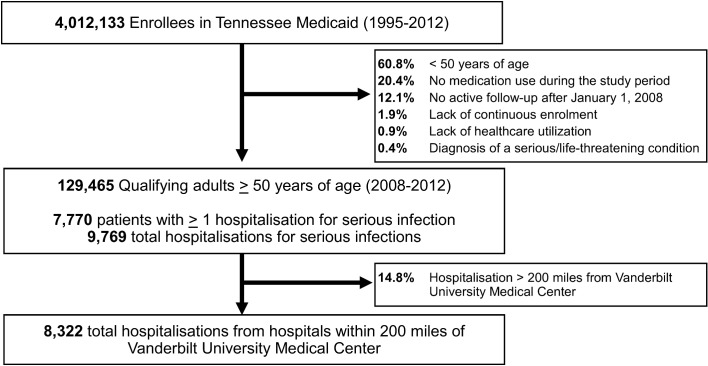
Setting and participants: We identified hospitalisations for possible infection among adults >=50 years enrolled in the Tennessee Medicaid healthcare programme (2008-2012) using International Classifications of Diseases, Ninth Revision diagnosis codes for pneumonia, meningitis/encephalitis, bacteraemia/sepsis, cellulitis/soft-tissue infections, endocarditis, pyelonephritis and septic arthritis/osteomyelitis.
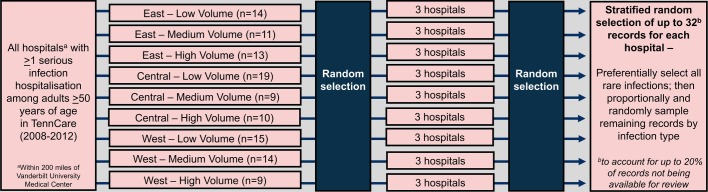
Design: Medical records were systematically obtained from hospitals randomly selected from a stratified sampling framework based on geographical region and hospital discharge volume.
Measures: Two trained clinical reviewers used a standardised extraction form to abstract information from medical records. Predefined algorithms served as reference to adjudicate confirmed infection-specific hospitalisations. We calculated the PPV of diagnosis codes using confirmed hospitalisations as reference. Sensitivity analyses determined the robustness of the PPV to definitions that required radiological or microbiological confirmation. We also determined inter-rater reliability between reviewers.
Results: The PPV of diagnosis codes for hospitalisations for infection (n=716) was 90.2% (95% CI 87.8% to 92.2%). The PPV was highest for pneumonia (96.5% (95% CI 93.9% to 98.0%)) and cellulitis (91.1% (95% CI 84.7% to 94.9%)), and lowest for meningitis/encephalitis (50.0% (95% CI 23.7% to 76.3%)). The adjudication reliability was excellent (92.7% agreement; first agreement coefficient: 0.91). The overall PPV was lower when requiring microbiological confirmation (45%) and when requiring radiological confirmation for pneumonia (79%).
Conclusions: Discharge diagnosis codes have a high PPV for identifying hospitalisations for common, serious infections among middle age and older adults. PPV estimates for rare infections were imprecise.
Keywords: coding algorithms; medicaid; older adults; serious infections.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: CGG has received consulting fees from Pfizer and Merck, and received research support from Sanofi-Pasteur, Campbell Alliance, the Centers for Disease Control and Prevention, National Institutes of Health, The Food and Drug Administration and the Agency for Health Care Research and Quality. WS has received personal fees from Pfizer, Merck, Novavax, Dynavax, Sanofi-Pasteur, GSK, Seqirus and received research support from the Centers for Disease Control and Prevention.
Figures
References
-
- Kim DK, Bridges CB, Harriman KH. Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP) ACIP Adult Immunization Work Group. Advisory committee on immunization practices recommended immunization schedule for adults aged 19 years or older--United States, 2015. MMWR Morb Mortal Wkly Rep 2015;64:214–2. 10.7326/M14-2755 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources