

Use of 4D Computer Tomographic Angiography to Accurately Identify Distal Internal Carotid Artery Occlusions and Pseudo-Occlusions: Technical Note
- PMID: 29922404
- PMCID: PMC5999302
Use of 4D Computer Tomographic Angiography to Accurately Identify Distal Internal Carotid Artery Occlusions and Pseudo-Occlusions: Technical Note
Abstract
Background and purpose: Traditional methods of computed tomographic angiography (CTA) can be unreliable in detecting carotid artery pseudo-occlusions or in accurately locating the site of carotid artery occlusion. With these methods, lack of adequate distal runoff due to pseudo-occlusion or intracranial occlusion can result in the inaccurate diagnoses of complete occlusion or cervical carotid occlusion, respectively. The site of carotid occlusion has important therapeutic and interventional considerations. We present several cases in which 4D CTA was utilized to accurately and noninvasively diagnose carotid pseudo-occlusion and intracranial internal carotid artery (ICA) occlusion.
Methods: We identified five patients who presented to our institute with ischemic stroke symptoms and evaluated images from traditional CTA protocols and 4D CTA protocols in each of these patients, comparing diagnoses rendered by each imaging technique.
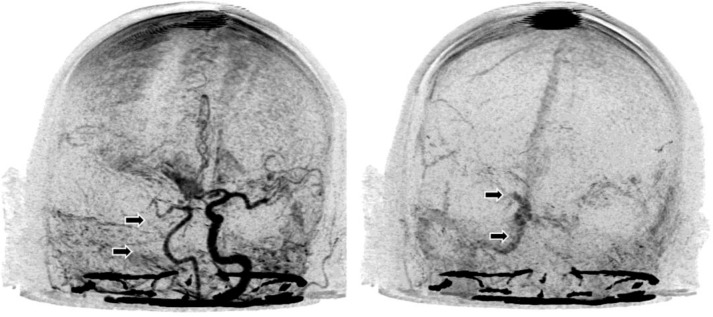
Results: In two patients, traditional CTA suggested the presence of complete ICA occlusion. However, 4D CTA demonstrated pseudo-occlusion. Similarly, in three patients, traditional CTA demonstrated cervical ICA occlusion, whereas the 4D CTA demonstrated intracranial ICA occlusion.
Conclusion: 4D CTA may be a more effective noninvasive imaging technique than traditional CTA to detect intracranial carotid artery occlusions and carotid artery pseudo-occlusions. Accurate, rapid, and noninvasive diagnosis of carotid artery lesions may help tailor and expedite endovascular intervention.
Keywords: carotid terminus occlusion; computed tomographic angiography; imaging; internal carotid artery; pseudo-occlusion.
Figures





Similar articles
-
Mid-cervical flame-shaped pseudo-occlusion: diagnostic performance of mid-cervical flame-shaped extracranial internal carotid artery sign on computed tomographic angiography in hyperacute ischemic stroke.Neuroradiology. 2017 Oct;59(10):989-996. doi: 10.1007/s00234-017-1882-3. Epub 2017 Aug 7. Neuroradiology. 2017. PMID: 28785800
-
Differentiating pseudo-occlusion from true occlusion of proximal internal carotid artery in acute ischemic stroke on CT angiography.Clin Neurol Neurosurg. 2019 Oct;185:105495. doi: 10.1016/j.clineuro.2019.105495. Epub 2019 Aug 19. Clin Neurol Neurosurg. 2019. PMID: 31470360
-
Perfusion-Derived Dynamic 4D CT Angiography Identifies Carotid Pseudo-Occlusion in Hyperacute Stroke.J Neuroimaging. 2016 Nov;26(6):588-591. doi: 10.1111/jon.12375. Epub 2016 Jul 7. J Neuroimaging. 2016. PMID: 27383381
-
Aetiologies of internal carotid artery pseudo-occlusions in acute stroke patients: what neurointerventionalists can expect.Br J Radiol. 2017 Feb;90(1070):20160352. doi: 10.1259/bjr.20160352. Epub 2016 Dec 20. Br J Radiol. 2017. PMID: 27995806 Free PMC article. Review.
-
Revascularization of tandem occlusions in acute ischemic stroke: review of the literature and illustrative case.Neurosurg Focus. 2017 Apr;42(4):E15. doi: 10.3171/2017.1.FOCUS16521. Neurosurg Focus. 2017. PMID: 28366063 Review.
References
-
- Kniemeyer HW, et al. Pseudo- and segmental occlusion of the internal carotid artery: a new classification, surgical treatment and results. Eur J Vasc Endovasc Surg. 1996;12:310–320. Available from: https://secureacademic.oup.com/licensing/index.html?doi=10.1093%252fons%.... - PubMed
-
- Siddiq F, et al. Occurrence and prognostic significance of cervical pseudodissection phenomenon associated with acute intracranial internal carotid artery occlusion. J Neuroimaging. 2013;23:384–390. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23228049. - PubMed
-
- Orrison WW, Jr, et al. Whole-brain dynamic CT angiography and perfusion imaging. Clin Radiol. 2011;66:566–574. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21371698. - PubMed
-
- Berkhemer OA, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25517348. - PubMed
-
- Furst G, et al. Reliability and validity of noninvasive imaging of internal carotid artery pseudo-occlusion. Stroke. 1999;30:1444–1449. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10390321. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous