

Invasive Aspergillosis Mimicking Metastatic Lung Cancer
- PMID: 29922593
- PMCID: PMC5996088
- DOI: 10.3389/fonc.2018.00188
Invasive Aspergillosis Mimicking Metastatic Lung Cancer
Abstract
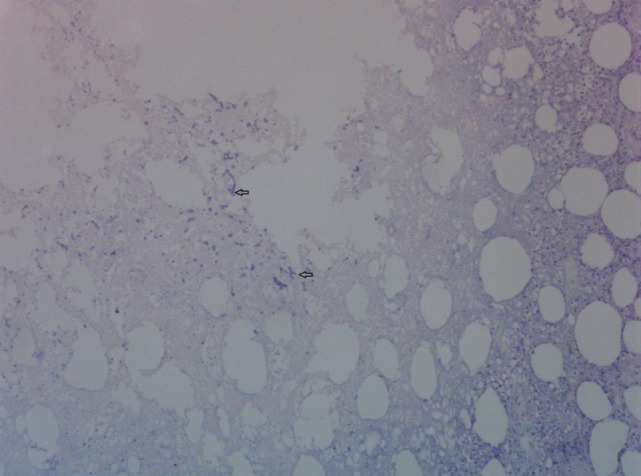
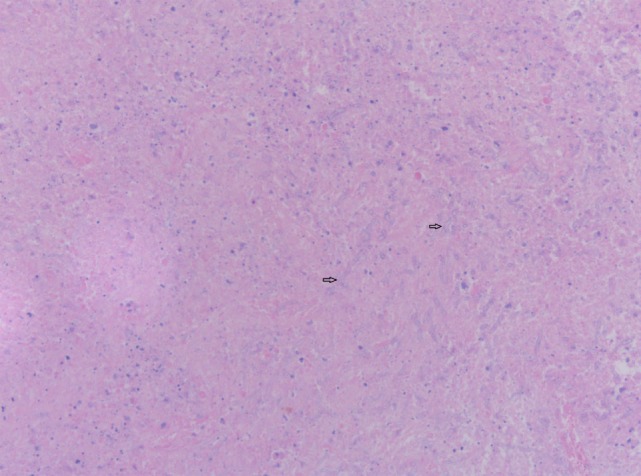
In a patient with a medical history of cancer, the most probable diagnosis of an 18FDG-avid pulmonary mass combined with intracranial abnormalities on brain imaging is metastasized cancer. However, sometimes a differential diagnosis with an infectious cause such as aspergillosis can be very challenging as both cancer and infection are sometimes difficult to distinguish. Pulmonary aspergillosis can present as an infectious pseudotumour with clinical and imaging characteristics mimicking lung cancer. Even in the presence of cerebral lesions, radiological appearance of abscesses can look like brain metastasis. These similarities can cause significant diagnostic difficulties with a subsequent therapeutic delay and a potential adverse outcome. Awareness of this infectious disease that can mimic lung cancer, even in an immunocompetent patient, is important. We report a case of a 65-year-old woman with pulmonary aspergillosis disseminated to the brain mimicking metastatic lung cancer.
Keywords: aspergillosis; brain abscess; brain metastasis; brain neoplasms; differential diagnosis; lung cancer; lung neoplasms.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources