

Short message service communication improves exclusive breastfeeding and early postpartum contraception in a low- to middle-income country setting: a randomised trial
- PMID: 29924912
- PMCID: PMC6179930
- DOI: 10.1111/1471-0528.15337
Short message service communication improves exclusive breastfeeding and early postpartum contraception in a low- to middle-income country setting: a randomised trial
Abstract
Objective: To assess the effect of short message service (SMS) communication on facility delivery, exclusive breastfeeding (EBF), and contraceptive use.
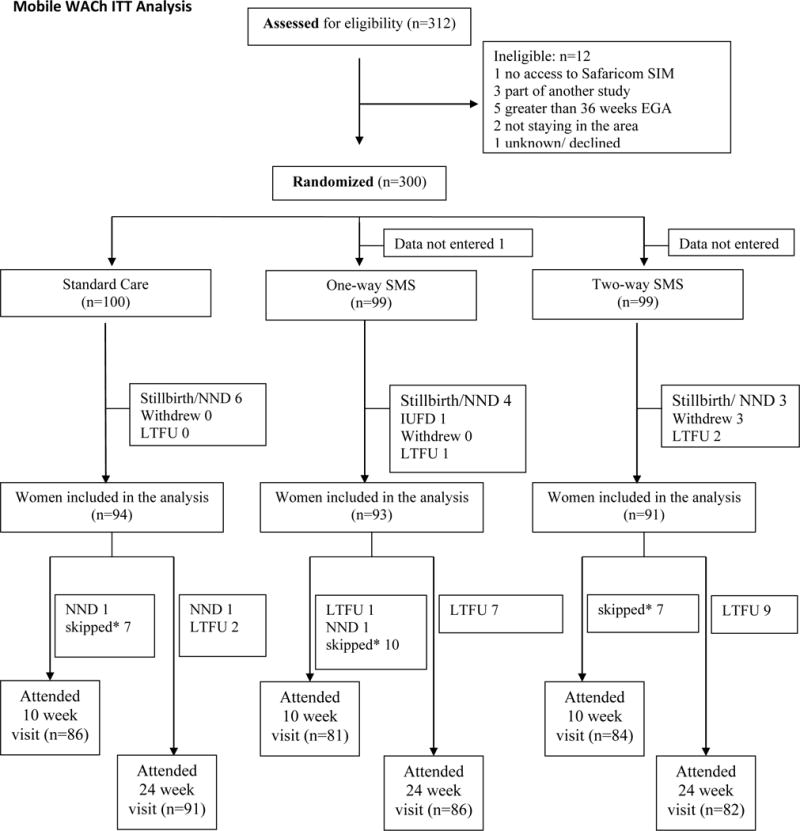
Design: Mobile WACh was a three-arm unblinded individually randomised controlled trial.
Setting: A public sector maternal child health (MCH) clinic in Nairobi, Kenya.
Population: Three hundred women attending antenatal care were randomised, 100 to each arm, and followed for 24 weeks postpartum. Pregnant women, at least 14 years old with access to a mobile phone and able to read SMS were eligible for participation.
Methods: Women were randomised (1:1:1) to receive one-way SMS versus two-way SMS with a nurse versus control. Weekly SMS content was tailored for maternal characteristics and pregnancy or postpartum timing.
Main outcome measures: Facility delivery, EBF, and contraceptive use were compared separately between each intervention arm and the control arm by Kaplan-Meier analysis and chi-square tests using intent-to-treat analyses.
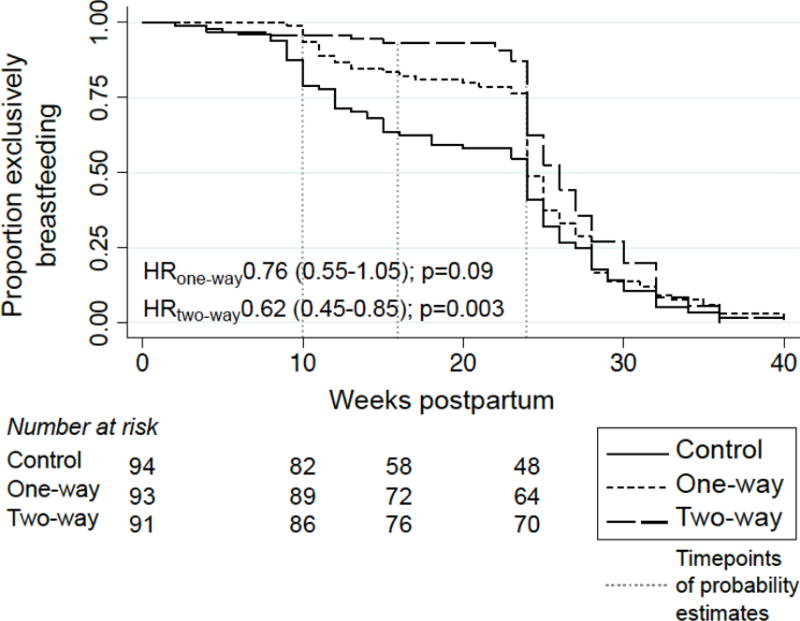
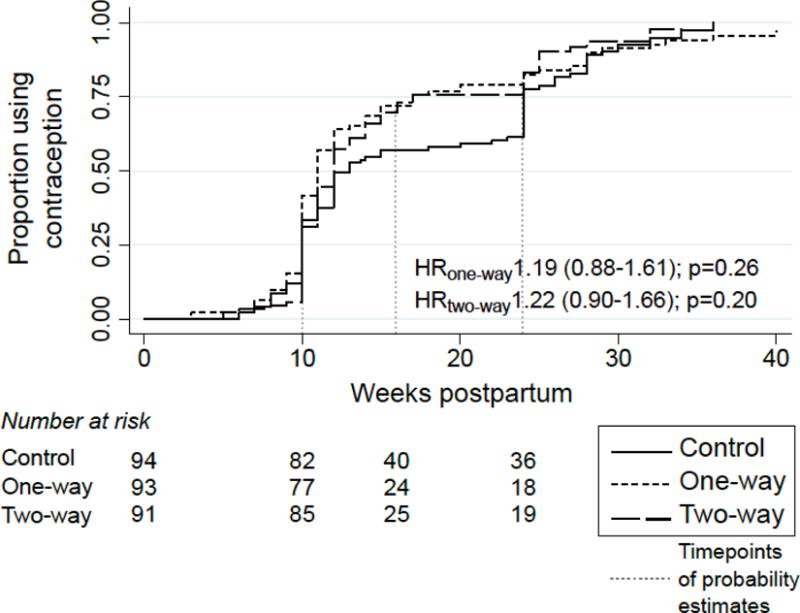
Results: The overall facility delivery rate was high (98%) and did not differ by arm. Compared with controls, probability of EBF was higher in the one-way SMS arm at 10 and 16 weeks, and in the two-way SMS arm at 10, 16, and 24 weeks (P < 0.005 for all). Contraceptive use was significantly higher in both intervention arms by 16 weeks (one-way SMS: 72% and two-way SMS: 73%; P = 0.03 and P = 0.02 versus 57% control, respectively); however, this difference was not significant when correcting for multiple comparisons.
Conclusion: One-way and two-way SMS improved EBF practices and early contraceptive use. Two-way SMS had an added benefit on sustained EBF, providing evidence that SMS messaging influences uptake of interventions that improve maternal and neonatal health.
Source of funding: Funding was provided by the National Institutes of Health (K12HD001264 to JAU, R01HD080460, K24HD054314 to GJS, and K01AI116298 to ALD), the National Science Foundation (Graduate Research Fellowship to TP and BD), as well as the University of Washington Global Center for Integrated Health of Women Adolescents and Children (Global WACh).
Tweetable abstract: The Mobile WACh RCT demonstrates that SMS improved practice of exclusive breastfeeding and early postpartum contraception.
Keywords: exclusive breastfeeding; facility delivery; family planning; mHealth; maternal child health.
© 2018 Royal College of Obstetricians and Gynaecologists.
Conflict of interest statement
The authors have no conflicts of interests to disclose. Completed disclosure of interest forms are available to view online as supporting information.
Figures
Comment in
-
Mobile phone innovations for maternal and neonatal health in low- and middle-income countries: the role of mHealth.BJOG. 2018 Nov;125(12):1630. doi: 10.1111/1471-0528.15345. Epub 2018 Aug 28. BJOG. 2018. PMID: 29927534 No abstract available.
References
-
- Nations U. Transforming our world: the 2030 Agenda for Sustainable Development. Sustainable Development Knowledge Platform. 2015
-
- Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet. 2016;387(10017):462–74. - PMC - PubMed
-
- Campbell OM, Graham WJ, Lancet Maternal Survival Series steering g Strategies for reducing maternal mortality: getting on with what works. Lancet. 2006;368(9543):1284–99. - PubMed
-
- Prata N, Sreenivas A, Vahidnia F, Potts M. Saving maternal lives in resource-poor settings: facing reality. Health Policy. 2009;89(2):131–48. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
