

Propofol attenuates the increase of sonographic optic nerve sheath diameter during robot-assisted laparoscopic prostatectomy: a randomized clinical trial
- PMID: 29925316
- PMCID: PMC6011519
- DOI: 10.1186/s12871-018-0523-7
Propofol attenuates the increase of sonographic optic nerve sheath diameter during robot-assisted laparoscopic prostatectomy: a randomized clinical trial
Abstract
Background: Robot-assisted laparoscopic prostatectomy (RALP) requires pneumoperitoneum and the Trendelenburg position to optimize surgical exposure, which can increase intracranial pressure (ICP). Anesthetic agents also influence ICP. We compared the effects of propofol and sevoflurane on sonographic optic nerve sheath diameter (ONSD) as a surrogate for ICP in prostate cancer patients who underwent RALP.
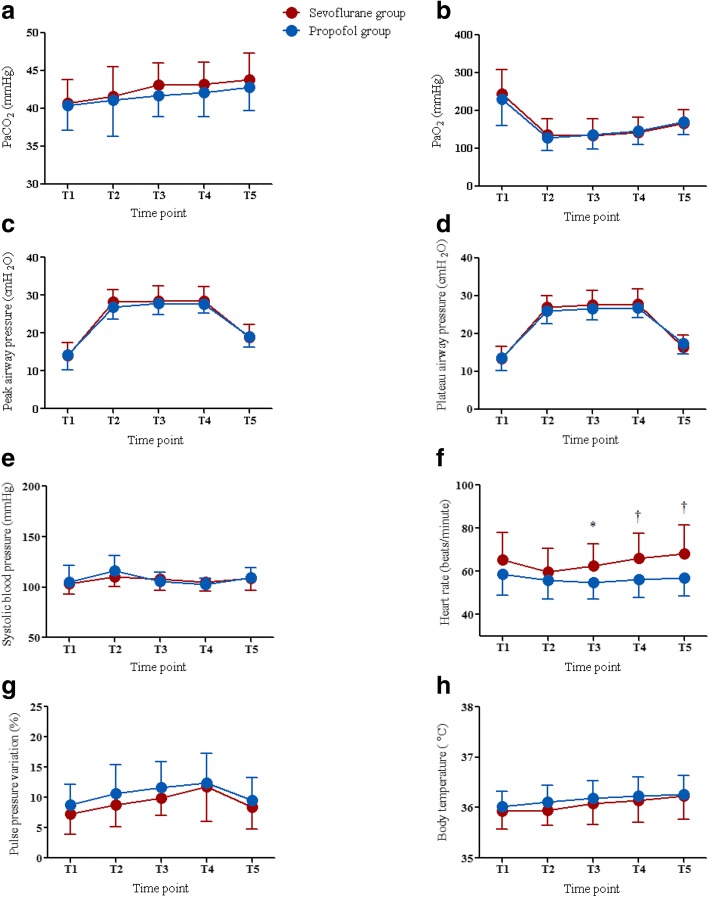
Methods: Thirty-six patients were randomly allocated to groups receiving propofol (propofol group, n = 18) or sevoflurane (sevoflurane group, n = 18) anesthesia. The ONSD was measured 10 min after induction of anesthesia in the supine position (T1); 5 min (T2), 30 min (T3), and 60 min (T4) after establishing pneumoperitoneum and the Trendelenburg position; and at the end of surgery after desufflation in the supine position (T5). Respiratory and hemodynamic variables were also evaluated.
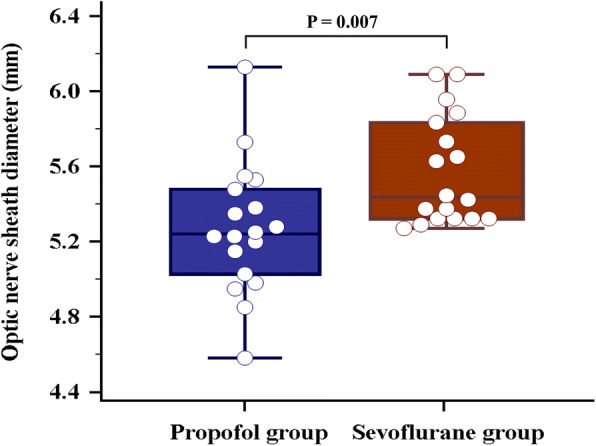
Results: The ONSD was significantly different between the propofol group and the sevoflurane group at T4 (5.27 ± 0.35 mm vs. 5.57 ± 0.28 mm, P = 0.007), but not at other time points. The ONSDs at T2, T3, T4, and T5 were significantly greater than at T1 in both groups (all P < 0.001). Arterial carbon dioxide partial pressure, arterial oxygen partial pressure, peak airway pressure, plateau airway pressure, systolic blood pressure, pulse pressure variation, body temperature and regional cerebral oxygen saturation, except heart rate, were not significantly different between the two groups.
Conclusions: The ONSD was significantly lower during propofol anesthesia than during sevoflurane anesthesia 60 min after pneumoperitoneum and the Trendelenburg position, suggesting that propofol anesthesia may help minimize ICP changes in robotic prostatectomy patients.
Trial registration: Clinicaltrials.gov identifier: NCT03271502 . Registered August 31, 2017.
Keywords: Propofol; Robot-assisted laparoscopic prostatectomy; Sevoflurane; Sonographic optic nerve sheath diameter.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Asan Medical Center Institutional Review Board (approval number: 2017–1011). Written informed consent was obtained from all patients.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Effect of Mannitol on Ultrasonographically Measured Optic Nerve Sheath Diameter as a Surrogate for Intracranial Pressure During Robot-Assisted Laparoscopic Prostatectomy with Pneumoperitoneum and the Trendelenburg Position.J Endourol. 2018 Jul;32(7):608-613. doi: 10.1089/end.2017.0828. Epub 2018 Mar 13. J Endourol. 2018. PMID: 29415565
-
Propofol Affects Optic Nerve Sheath Diameter less than Sevoflurane during Robotic Surgery in the Steep Trendelenburg Position.Biomed Res Int. 2019 Dec 14;2019:5617815. doi: 10.1155/2019/5617815. eCollection 2019. Biomed Res Int. 2019. PMID: 31915696 Free PMC article. Clinical Trial.
-
Sonographic optic nerve sheath diameter as a surrogate measure for intracranial pressure in anesthetized patients in the Trendelenburg position.BMC Anesthesiol. 2015 Mar 31;15:43. doi: 10.1186/s12871-015-0025-9. eCollection 2015. BMC Anesthesiol. 2015. PMID: 25861241 Free PMC article.
-
Effects of propofol and inhalational anesthetics on the optic nerve sheath diameter in patients undergoing surgery in the steep Trendelenburg position: a systematic review and meta-analysis.Ann Palliat Med. 2021 Oct;10(10):10475-10485. doi: 10.21037/apm-21-2363. Ann Palliat Med. 2021. PMID: 34763494
-
Ultrasonographic optic nerve sheath diameter for predicting elevated intracranial pressure during laparoscopic surgery: a systematic review and meta-analysis.Surg Endosc. 2018 Jan;32(1):175-182. doi: 10.1007/s00464-017-5653-3. Epub 2017 Jun 21. Surg Endosc. 2018. PMID: 28639043
Cited by
-
Optic nerve sheath diameter changes during gynecologic surgery in the Trendelenburg position: comparison of propofol-based total intravenous anesthesia and sevoflurane anesthesia.Anesth Pain Med (Seoul). 2019 Oct 31;14(4):393-400. doi: 10.17085/apm.2019.14.4.393. Anesth Pain Med (Seoul). 2019. PMID: 33329767 Free PMC article.
-
Intelligent medicine in focus: the 5 stages of evolution in robot-assisted surgery for prostate cancer in the past 20 years and future implications.Mil Med Res. 2024 Aug 21;11(1):58. doi: 10.1186/s40779-024-00566-z. Mil Med Res. 2024. PMID: 39164787 Free PMC article. Review.
-
Effect of sevoflurane, propofol and propofol with dexmedetomidine as maintenance agent on intracranial pressure in the Trendelenburg position during laparoscopic surgeries.J Anaesthesiol Clin Pharmacol. 2023 Jul-Sep;39(3):474-481. doi: 10.4103/joacp.joacp_511_21. Epub 2023 Sep 29. J Anaesthesiol Clin Pharmacol. 2023. PMID: 38025555 Free PMC article.
-
The effect of laryngoscope types on hemodynamic response and optic nerve sheath diameter. McCoy, Macintosh, and C-MAC video-laryngoscope.Saudi Med J. 2020 Sep;41(9):930-937. doi: 10.15537/smj.2020.9.25349. Saudi Med J. 2020. PMID: 32893274 Free PMC article. Clinical Trial.
-
Dexmedetomidine attenuates the increase of ultrasonographic optic nerve sheath diameter as a surrogate for intracranial pressure in patients undergoing robot-assisted laparoscopic prostatectomy: A randomized double-blind controlled trial.Medicine (Baltimore). 2019 Aug;98(33):e16772. doi: 10.1097/MD.0000000000016772. Medicine (Baltimore). 2019. PMID: 31415378 Free PMC article. Clinical Trial.
References
-
- Gainsburg DM. Anesthetic concerns for robotic-assisted laparoscopic radical prostatectomy. Minerva Anestesiol. 2012;78(5):596–604. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
