

Development, modelling, and pilot testing of a complex intervention to support end-of-life care provided by Danish general practitioners
- PMID: 29925332
- PMCID: PMC6011239
- DOI: 10.1186/s12875-018-0774-x
Development, modelling, and pilot testing of a complex intervention to support end-of-life care provided by Danish general practitioners
Abstract
Background: Most patients in end-of-life with life-threatening diseases prefer to be cared for and die at home. Nevertheless, the majority die in hospitals. GPs have a pivotal role in providing end-of-life care at patients' home, and their involvement in the palliative trajectory enhances the patient's possibility to stay at home. The aim of this study was to develop and pilot-test an intervention consisting of continuing medical education (CME) and electronic decision support (EDS) to support end-of-life care in general practice.
Methods: We developed an intervention in line with the first phases of the guidelines for complex interventions drawn up by the Medical Research Council. Phase 1 involved the development of the intervention including identification of key barriers to provision of end-of-life care for GPs and of facilitators of change. Furthermore the actual modelling of two components: CME meeting and EDS. Phase 2 focused on pilot-testing and intervention assessment by process evaluation.
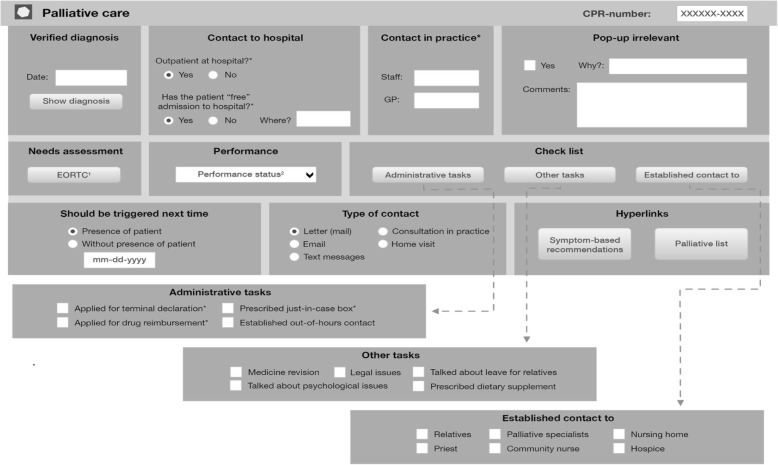
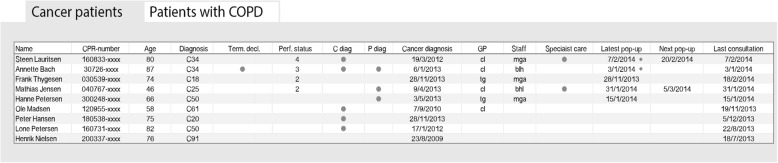
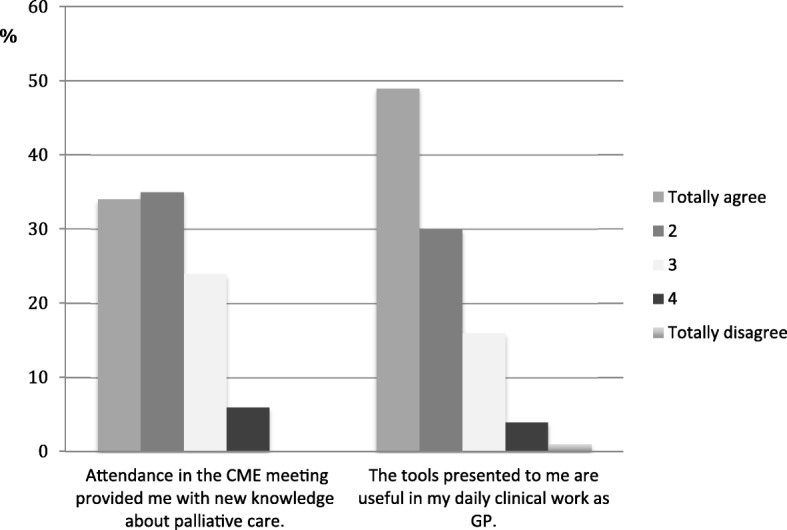
Results: In phase 1 lack of identification of patients at the end of life and limited palliative knowledge among GPs were identified as barriers. The CME meeting and the EDS were developed. The CME meeting was a four-hour educational meeting performed by GPs and specialists in palliative care. The EDS consisted of two parts: a pop-up window for each patient with palliative needs and a list of all patients with palliative needs in the practice. The pilot testing in phase 2 showed that the CME meeting was performed as intended and 120 (14%) of the GPs in the region attended. The EDS was integrated in existing electronic records but was shut down early for external reasons; 50 (5%) GPs signed up. The pilot-testing demonstrated a need to strengthen the implementation as attending rate was low in the current set-up.
Conclusion: We developed a complex intervention to support GPs in providing end-of-life care. The pilot-test showed general acceptance of the CME meetings. The EDS was shut down early and needs further evaluation before examining the whole intervention in a larger study, where evaluation could be based on patient-related outcomes and impact on end-of-life care.
Trial registration: Clinicaltrials.gov ( NCT02050256 ) January 30, 2014.
Keywords: COPD; Cancer; Clinical decision support systems; Complex intervention; Continuing medical education; Denmark; End-of-life care; General practice; Palliative care.
Conflict of interest statement
Ethics approval and consent to participate
According to the Committee on Health Research Ethics of the Central Denmark Region, the Danish Act on Research Ethics Review of Health Research Projects does not apply to this project (file no. 31/201). The study was approved by the Danish Data Protection Agency (J.no. 2013–41-1965) and was registered in clinicaltrials.gov (NCT02050256).
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Increasing the chance of dying at home: roles, tasks and approaches of general practitioners enabling palliative care: a systematic review of qualitative literature.BMC Prim Care. 2023 Mar 23;24(1):77. doi: 10.1186/s12875-023-02038-0. BMC Prim Care. 2023. PMID: 36959553 Free PMC article.
-
Patient-centeredness to anticipate and organize an end-of-life project for patients receiving at-home palliative care: a phenomenological study.BMC Fam Pract. 2017 Feb 23;18(1):27. doi: 10.1186/s12875-017-0602-8. BMC Fam Pract. 2017. PMID: 28231821 Free PMC article.
-
"It is not the fading candle that one expects": general practitioners' perspectives on life-preserving versus "letting go" decision-making in end-of-life home care.Scand J Prim Health Care. 2015;33(4):233-42. doi: 10.3109/02813432.2015.1118837. Epub 2015 Dec 10. Scand J Prim Health Care. 2015. PMID: 26654583 Free PMC article.
-
Belgian general practitioners' perspectives on the use of palliative sedation in end-of-life home care: a qualitative study.J Pain Symptom Manage. 2014 Jun;47(6):1054-63. doi: 10.1016/j.jpainsymman.2013.06.016. Epub 2013 Oct 2. J Pain Symptom Manage. 2014. PMID: 24095283
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
Cited by
-
Digital solutions for decision support in general practice - a rapid review focused on systems developed for the universal healthcare setting in Denmark.BMC Prim Care. 2023 Dec 14;24(1):276. doi: 10.1186/s12875-023-02234-y. BMC Prim Care. 2023. PMID: 38097998 Free PMC article. Review.
-
Increasing the chance of dying at home: roles, tasks and approaches of general practitioners enabling palliative care: a systematic review of qualitative literature.BMC Prim Care. 2023 Mar 23;24(1):77. doi: 10.1186/s12875-023-02038-0. BMC Prim Care. 2023. PMID: 36959553 Free PMC article.
-
Clinical Decision Support and Implications for the Clinician Burnout Crisis.Yearb Med Inform. 2020 Aug;29(1):145-154. doi: 10.1055/s-0040-1701986. Epub 2020 Aug 21. Yearb Med Inform. 2020. PMID: 32823308 Free PMC article. Review.
-
Evaluation of the Acute Basic Palliation Concept by Relatives and Health Care Professionals: An Observational Study of 40 Home-Dying Patients in Denmark.Palliat Med Rep. 2025 Feb 1;6(1):6-16. doi: 10.1089/pmr.2024.0062. Epub 2025 Feb 5. Palliat Med Rep. 2025. PMID: 40160721 Free PMC article.
References
-
- Definition of General Practice, EURACT (short version, 2011). [http://www.woncaeurope.org/sites/default/files/documents/Definition EURA...] 28 March 2014.
-
- Michiels E, Deschepper R, Van Der Kelen G, Bernheim JL, Mortier F, Vander Stichele R, Deliens L. The role of general practitioners in continuity of care at the end of life: a qualitative study of terminally ill patients and their next of kin. Palliat Med. 2007;21(5):409–415. doi: 10.1177/0269216307078503. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
