

Liver maximum capacity (LiMAx) test as a helpful prognostic tool in acute liver failure with sepsis: a case report
- PMID: 29925334
- PMCID: PMC6011251
- DOI: 10.1186/s12871-018-0538-0
Liver maximum capacity (LiMAx) test as a helpful prognostic tool in acute liver failure with sepsis: a case report
Abstract
Background: Acute liver failure (ALF) is a life-threatening entity particularly when infectious complications worsen the clinical course. Urgent liver transplantation (LT) is frequently the only curative treatment. However, in some cases, recovery is observed under conservative treatment. Therefore, prognostic tools for estimating course of the disease are of great clinical interest. Since laboratory parameters sometimes lack sensitivity and specificity, enzymatic liver function measured by liver maximum capacity (LiMAx) test may offer novel and valuable additional information in this setting.
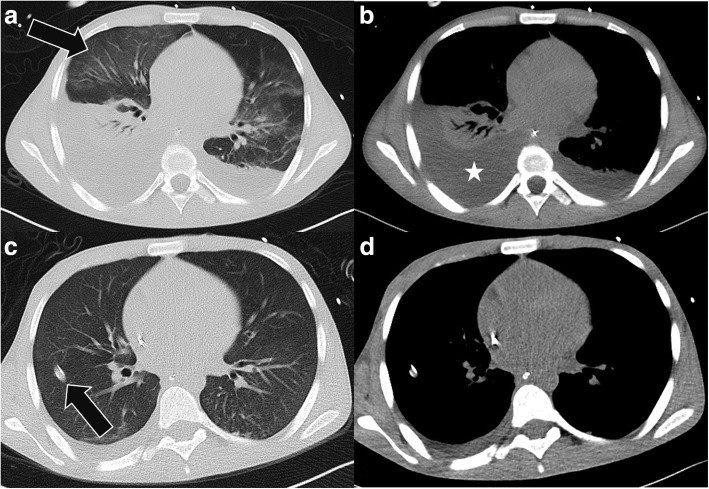
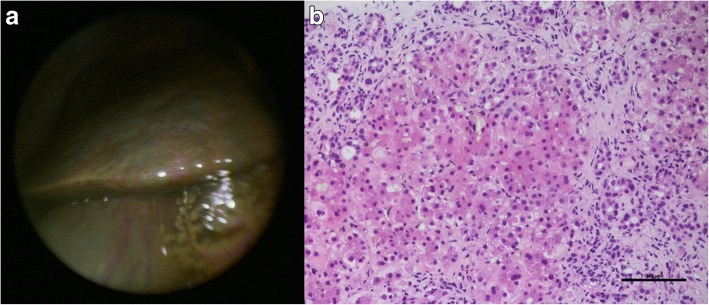
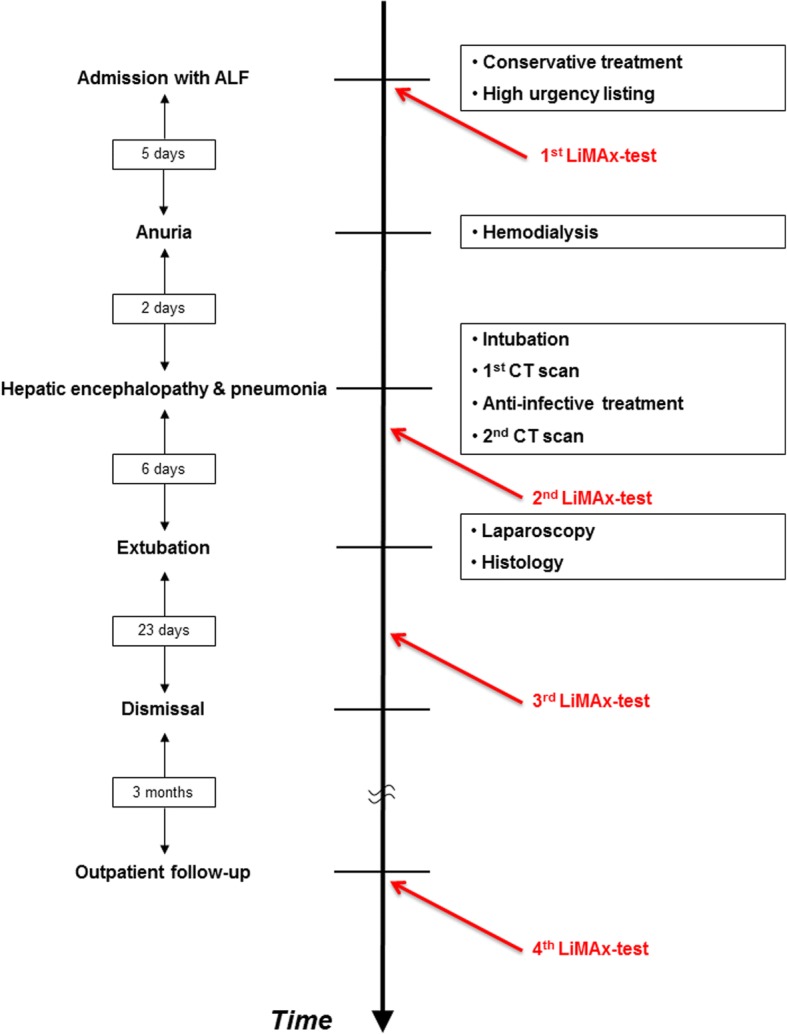
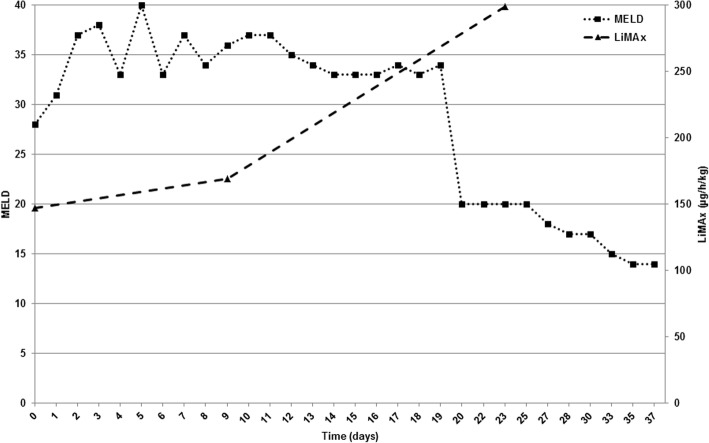
Case presentation: We here report the case of a formerly healthy 20-year old male caucasian patient who was admitted to our clinic for ALF of unknown origin in December 2017. Laboratory parameters confirmed the diagnosis with an initial MELD score of 28 points. Likewise, enzymatic liver function was significantly impaired with a value of 147 [> 315] μg/h/kg. Clinical and biochemical analyses for viral-, autoimmune-, or drug-induced hepatitis were negative. Liver synthesis parameters further deteriorated reaching a MELD score of 40 points whilst clinical course was complicated by septic pneumonia leading to severe hepatic encephalopathy grade III-IV, finally resulting in mechanical ventilation of the patient. Interestingly, although clinical course and laboratory data suggested poor outcome, serial LiMAx test revealed improvement of the enzymatic liver function at this time point increasing to 169 μg/h/kg. Clinical condition and laboratory data slowly improved likewise, however with significant time delay of 11 days. Finally, the patient could be dismissed from our clinic after 37 days.
Conclusion: Estimating prognosis in patients with ALF is challenging by use of the established scores. In our case, improvement of enzymatic liver function measured by the LiMAx test was the first parameter predicting beneficial outcome in a patient with ALF complicated by sepsis.
Keywords: Acute liver failure; King’s college criteria; LiMAx; Liver transplantation; MELD score.
Conflict of interest statement
Ethics approval and consent to participate
The ethics committee of the University of Duisburg-Essen (“Ethik-Kommission der Medizinischen Fakultät der Universität Duisburg-Essen”, Director Prof. Dr. U. Schara) approved the anonymous collection and publication of data for this case report.
Consent for publication
Written informed consent was obtained from the participant for publication of this article and any accompanying tables/images. A copy of the written consent is available for review by the Editor of this journal. The abstract was presented at the 27th annual congress of the “Gesellschaft für Gastroenterologie in Nordrhein-Westfalen” on 7th/8th june 2018 (Gastroenterologe (2018) 13: 215. 10.1007/s11377-018-0258-5). Permission from the copyright holder was obtained.
Competing interests
MB received consultant fee from Humedics. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Predicting the prognosis in acute liver failure: results from a retrospective pilot study using the LiMAx test.Ann Hepatol. 2013 Jul-Aug;12(4):556-62. Ann Hepatol. 2013. PMID: 23813133
-
Indocyanine green clearance test combined with MELD score in predicting the short-term prognosis of patients with acute liver failure.Hepatobiliary Pancreat Dis Int. 2014 Jun;13(3):271-5. doi: 10.1016/s1499-3872(14)60040-0. Hepatobiliary Pancreat Dis Int. 2014. PMID: 24919610
-
[Clinical features of patients with fulminant hepatitis A requiring emergency liver transplantation: comparison with acute liver failure due to other causes].Korean J Hepatol. 2010 Mar;16(1):19-28. doi: 10.3350/kjhep.2010.16.1.19. Korean J Hepatol. 2010. PMID: 20375639 Korean.
-
LDH and the MELD-LDH in Severe Acute Liver Injury and Acute Liver Failure: Preliminary Confirmation of a Novel Prognostic Score for Risk Stratification.J Appl Lab Med. 2023 May 4;8(3):504-513. doi: 10.1093/jalm/jfac137. J Appl Lab Med. 2023. PMID: 36759930 Review.
-
Ability of King's College Criteria and Model for End-Stage Liver Disease Scores to Predict Mortality of Patients With Acute Liver Failure: A Meta-analysis.Clin Gastroenterol Hepatol. 2016 Apr;14(4):516-525.e5; quiz e43-e45. doi: 10.1016/j.cgh.2015.10.007. Epub 2015 Oct 20. Clin Gastroenterol Hepatol. 2016. PMID: 26499930 Review.
Cited by
-
Enzymatic liver function measured by LiMAx - a reliable diagnostic and prognostic tool in chronic liver disease.Sci Rep. 2019 Sep 19;9(1):13577. doi: 10.1038/s41598-019-49746-1. Sci Rep. 2019. PMID: 31537822 Free PMC article.
-
[Hepatic dysfunction in patients with cardiogenic shock].Med Klin Intensivmed Notfmed. 2019 Oct;114(7):665-676. doi: 10.1007/s00063-019-00618-6. Epub 2019 Sep 19. Med Klin Intensivmed Notfmed. 2019. PMID: 31538212 Review. German.
-
Profound decrease of liver maximum function capacity test of isoflurane sedated patients: A report of three cases.Clin Case Rep. 2021 Sep 24;9(9):e04862. doi: 10.1002/ccr3.4862. eCollection 2021 Sep. Clin Case Rep. 2021. PMID: 34594555 Free PMC article.
-
Immunomodulation by Hemoadsorption-Changes in Hepatic Biotransformation Capacity in Sepsis and Septic Shock: A Prospective Study.Biomedicines. 2022 Sep 20;10(10):2340. doi: 10.3390/biomedicines10102340. Biomedicines. 2022. PMID: 36289602 Free PMC article.
-
Dosing of Antimycotic Treatment in Sepsis-Induced Liver Dysfunction by Functional Liver Testing with LiMAx®.Case Rep Crit Care. 2019 Dec 26;2019:5362514. doi: 10.1155/2019/5362514. eCollection 2019. Case Rep Crit Care. 2019. PMID: 31949955 Free PMC article.
References
-
- Polson J, Lee WM. American Association for the Study of liver disease. AASLD position paper: the management of acute liver failure Hepatol Baltim Md. 2005;41:1179–1197. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
