

Treatment outcomes in metastatic and localized high-grade salivary gland cancer: high chance of cure with surgery and post-operative radiation in T1-2 N0 high-grade salivary gland cancer
- PMID: 29925355
- PMCID: PMC6011413
- DOI: 10.1186/s12885-018-4578-0
Treatment outcomes in metastatic and localized high-grade salivary gland cancer: high chance of cure with surgery and post-operative radiation in T1-2 N0 high-grade salivary gland cancer
Abstract
Background: High-grade salivary gland cancer is a distinct clinical entity that has aggressive disease progression and early systemic spread. However, because of the rarity of the disease, the clinical outcomes, prognostic factors and clinical decision on the optimal treatments have not been fully understood.
Methods: In this study, we retrospectively analyzed the clinical data of 124 patients with high-grade salivary gland cancers and performed multivariate survival analyses to evaluate the clinico-pathological factors affecting the treatment outcomes.
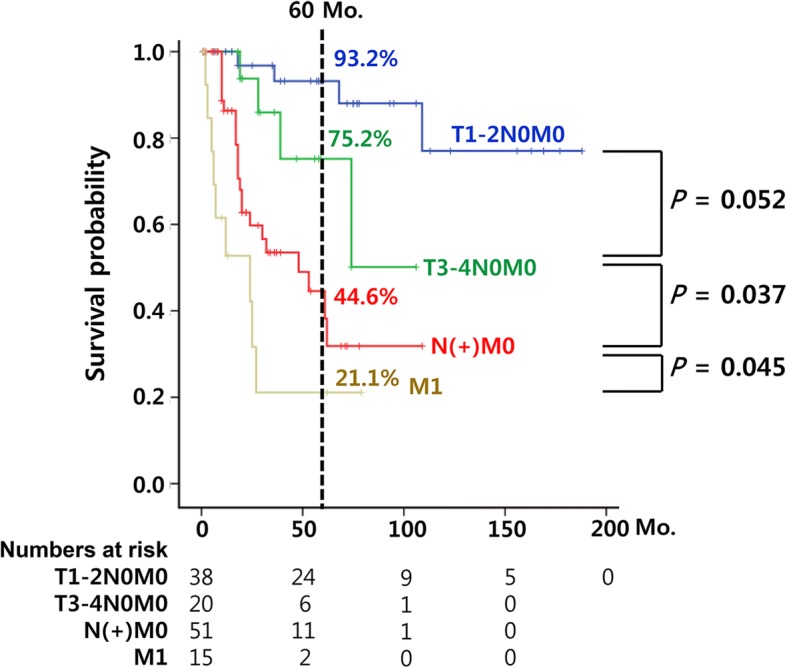
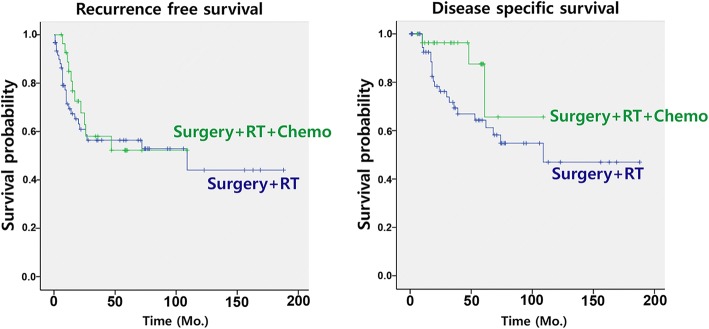
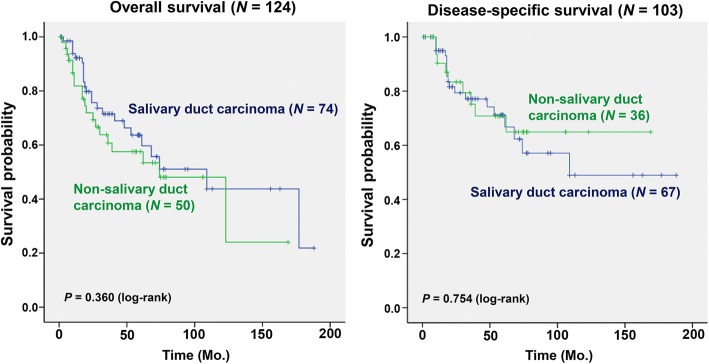
Results: The 5-year disease-specific survival was 63.4% in patients with high-grade salivary gland cancers. Among the clinico-pathological factors, presence of lymph node metastasis (hazard ratio 5.63, 95% confidence interval 2.64-12.03, P < 0.001) and distant metastasis (hazard ratio 4.59, 95% confidence interval 2.10-10.04, P < 0.001) at diagnosis were the most potent unfavorable prognostic factors. Importantly, patients with early-stage disease (T1-2N0M0) showed apparently a relatively excellent prognosis (93.2% 5-year disease-specific survival); meanwhile N (+) and M1 status at diagnosis resulted in dismal outcomes (44.6 and 21.1% 5-year disease-specific survival, respectively). On comparing surgery alone as a treatment modality, surgery plus postoperative radiation significantly benefited the patients, but the difference between adjuvant radiation and chemoradiation was not found to be significant. Pathological subtypes of high-grade salivary gland cancers were not significantly associated with prognosis.
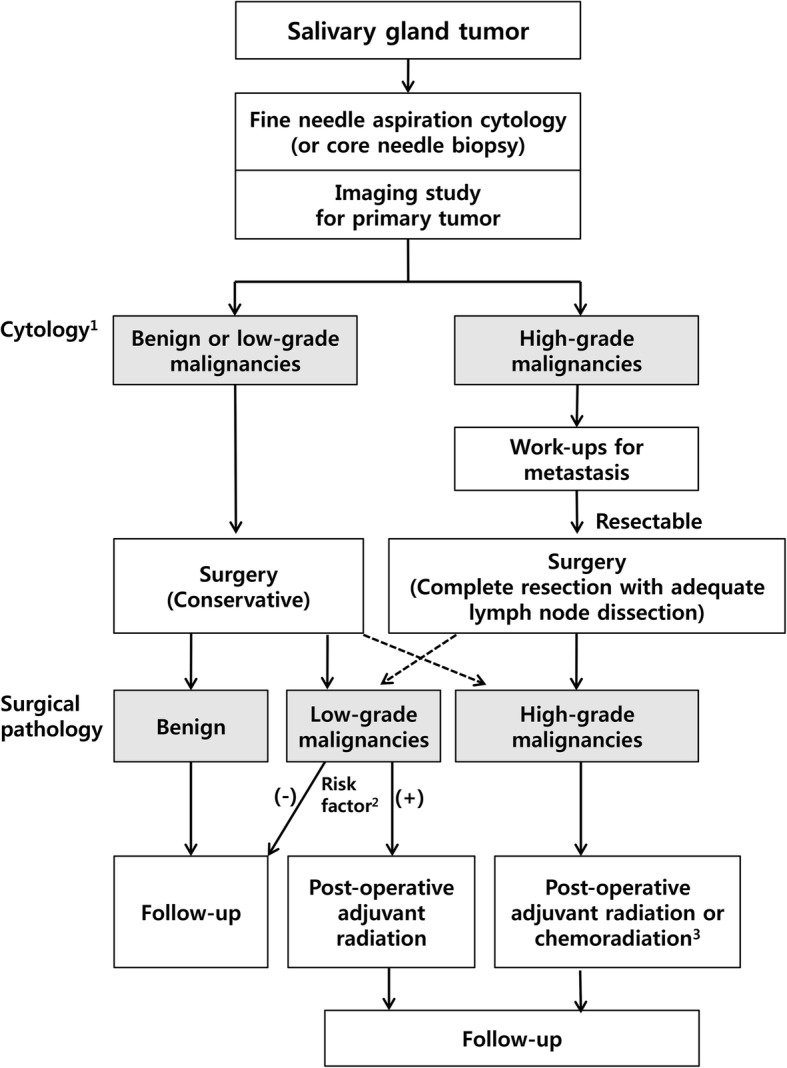
Conclusions: Despite of an overall unfavorable prognosis in high-grade salivary gland cancer, patients with early-stage disease are expected to have excellent prognosis (over 90% survival rates) with surgery plus adjuvant radiation, which may implicate the patients' consultation, therapeutic decision making, and the need for early detection of the disease.
Keywords: High-grade pathology; Prognosis; Salivary gland neoplasm; Treatment outcomes.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of Samsung Medical Center. The written informed consent was not required for this retrospective study. The data used in this study was de-identified.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- El-Naggar AK. Tumours of salivary glands. In: El-Naggar AK, JKC C, Grandis JR, Takata T, Slootweg PJ, editors. WHO Classification of Head and Neck Tumours. Lyon, France: WHO Press; 2017. pp. 159–202.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
