The Impact of Implementation of a Clinically Integrated Problem-Based Neonatal Electronic Health Record on Documentation Metrics, Provider Satisfaction, and Hospital Reimbursement: A Quality Improvement Project
- PMID: 29925495
- PMCID: PMC6031895
- DOI: 10.2196/medinform.9776
The Impact of Implementation of a Clinically Integrated Problem-Based Neonatal Electronic Health Record on Documentation Metrics, Provider Satisfaction, and Hospital Reimbursement: A Quality Improvement Project
Abstract
Background: A goal of effective electronic health record provider documentation platforms is to provide an efficient, concise, and comprehensive notation system that will effectively reflect the clinical course, including the diagnoses, treatments, and interventions.
Objective: The aim is to fully redesign and standardize the provider documentation process, seeking improvement in documentation based on ongoing All Patient Refined Diagnosis Related Group-based coding records, while maintaining noninferiority comparing provider satisfaction to our existing documentation process. We estimated the fiscal impact of improved documentation based on changes in expected hospital payments.
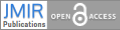
Methods: Employing a multidisciplinary collaborative approach, we created an integrated clinical platform that captures data entry from the obstetrical suite, delivery room, neonatal intensive care unit (NICU) nursing and respiratory therapy staff. It provided the sole source for hospital provider documentation in the form of a history and physical exam, daily progress notes, and discharge summary. Health maintenance information, follow-up appointments, and running contemporaneous updated hospital course information have selected shared entry and common viewing by the NICU team. The interventions were to (1) improve provider awareness of appropriate documentation through a provider education handout and follow-up group discussion and (2) fully redesign and standardize the provider documentation process building from the native Epic-based software. The measures were (1) hospital coding department review of all NICU admissions and 3M All Patient Refined Diagnosis Related Group-based calculations of severity of illness, risk of mortality, and case mix index scores; (2) balancing measure: provider time utilization case study and survey; and (3) average expected hospital payment based on acuity-based clinical logic algorithm and payer mix.
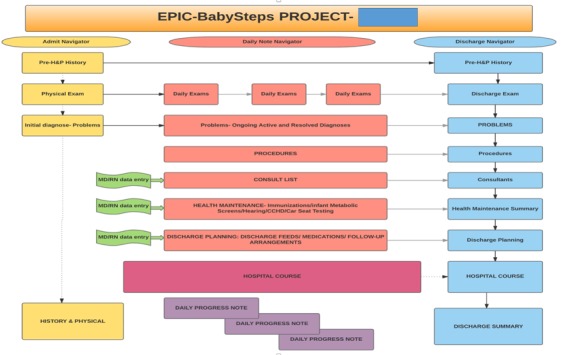
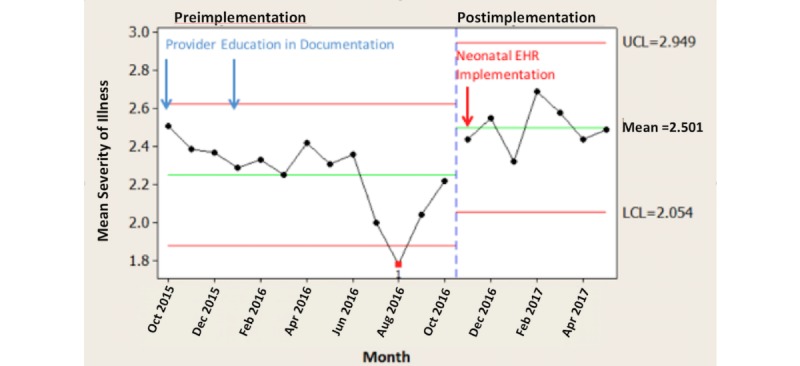
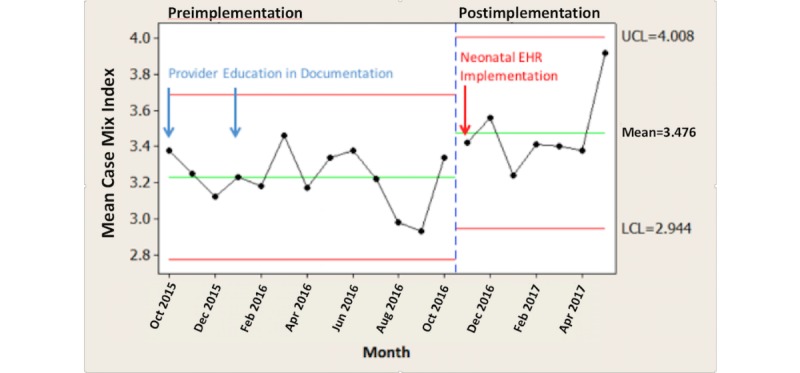
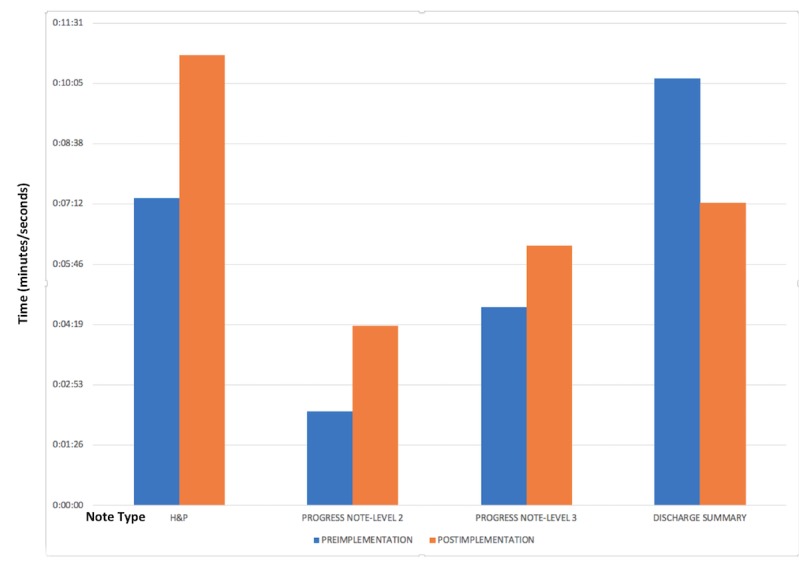
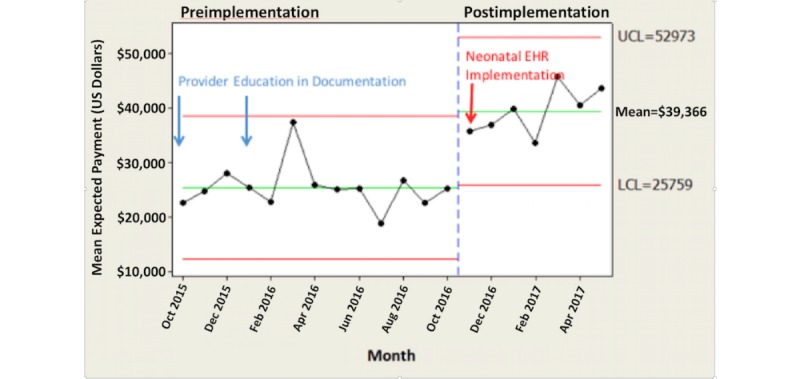
Results: We compared preintervention (October 2015-October 2016) to postintervention (November 2016-May 2017) time periods and saw: (1) significant improvement in All Patient Refined Diagnosis Related Group-derived severity of illness, risk of mortality, and case mix index (monthly average severity of illness scores increased by 11.1%, P=.008; monthly average risk of mortality scores increased by 13.5%, P=.007; and monthly average case mix index scores increased by 7.7%, P=.009); (2) time study showed increased time to complete history and physical and progress notes and decreased time to complete discharge summary (history and physical exam: time allocation increased by 47%, P=.05; progress note: time allocation increased by 91%, P<.001; discharge summary: time allocation decreased by 41%, P=.03); (3) survey of all providers: overall there was positive provider perception of the new documentation process based on a survey of the provider group; (4) significantly increased hospital average expected payments: comparing the preintervention and postintervention study periods, there was a US $14,020 per month per patient increase in average expected payment for hospital charges (P<.001). There was no difference in payer mix during this time period.
Conclusions: A problem-based NICU documentation electronic health record more effectively improves documentation without dissatisfaction by the participating providers and improves hospital estimations of All Patient Refined Diagnosis Related Group-based revenue.
Keywords: APR-DRG; CMI; Epic; NICU; ROM; SOI; electronic health record; informatics; neonatal intensive care unit; physician documentation.
©William Liu, Thomas Walsh. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 20.06.2018.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Implementation of a Clinical Documentation Improvement Curriculum Improves Quality Metrics and Hospital Charges in an Academic Surgery Department.J Am Coll Surg. 2017 Mar;224(3):301-309. doi: 10.1016/j.jamcollsurg.2016.11.010. Epub 2016 Dec 2. J Am Coll Surg. 2017. PMID: 27919741
-
Impact of improved documentation on an academic neurosurgical practice.J Neurosurg. 2014 Mar;120(3):756-63. doi: 10.3171/2013.11.JNS13852. Epub 2013 Dec 20. J Neurosurg. 2014. PMID: 24359011
-
[Implementation of a patient data management system. Effects on intensive care documentation].Anaesthesist. 2013 Nov;62(11):887-90, 892-7. doi: 10.1007/s00101-013-2239-x. Epub 2013 Oct 16. Anaesthesist. 2013. PMID: 24126951 German.
-
Clinical Documentation for Intensivists: The Impact of Diagnosis Documentation.Crit Care Med. 2020 Apr;48(4):579-587. doi: 10.1097/CCM.0000000000004200. Crit Care Med. 2020. PMID: 32205605 Review.
-
Review of medical discharge summaries and medical documentation in a metropolitan hospital: impact on diagnostic-related groups and Weighted Inlier Equivalent Separation.Intern Med J. 2013 Jul;43(7):767-71. doi: 10.1111/imj.12084. Intern Med J. 2013. PMID: 23347364 Review.
Cited by
-
Problem-oriented documentation: design and widespread adoption of a novel toolkit in a commercial electronic health record.JAMIA Open. 2023 Feb 3;6(1):ooad005. doi: 10.1093/jamiaopen/ooad005. eCollection 2023 Apr. JAMIA Open. 2023. PMID: 36751467 Free PMC article.
-
Standardized Neonatal ICU Progress Note Template and Feedback System: A Clinical Documentation Improvement Initiative.Cureus. 2024 Dec 8;16(12):e75309. doi: 10.7759/cureus.75309. eCollection 2024 Dec. Cureus. 2024. PMID: 39776738 Free PMC article.
-
Implementation of a Provider's Asthma-specific Note to Optimize Billing in the Pediatric Emergency Department.Pediatr Qual Saf. 2022 Mar 30;7(2):e544. doi: 10.1097/pq9.0000000000000544. eCollection 2022 Mar-Apr. Pediatr Qual Saf. 2022. PMID: 35369414 Free PMC article.
-
Linking household members and defining relational networks using routine health data.Curr Opin Pediatr. 2025 Feb 1;37(1):27-33. doi: 10.1097/MOP.0000000000001415. Epub 2024 Nov 4. Curr Opin Pediatr. 2025. PMID: 39509188 Review.
-
MedCDI: A technology-based documentation and quality improvement initiative in neurosurgery.Surg Neurol Int. 2022 Jun 23;13:271. doi: 10.25259/SNI_454_2022. eCollection 2022. Surg Neurol Int. 2022. PMID: 35855135 Free PMC article.
References
-
- Sebelius K. Federal Register. 2009. Oct 09, [2017-12-13]. Department of Health and Human Services: Health Information Technology for Economic and Clinical Health Act https://www.hhs.gov/sites/default/files/ocr/privacy/hipaa/administrative... .
-
- Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, Roth E, Morton SC, Shekelle PG. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742–752.0000605-200605160-00125 - PubMed
-
- Meinert DB. Resistance to electronic medical records (EMRs): a barrier to improved quality of care. IISIT. 2005;2:494–504. doi: 10.28945/846. - DOI
-
- Ajami S, Bagheri-Tadi T. Barriers for adopting electronic health records (EHRs) by physicians. Acta Inform Med. 2013;21(2):129–134. doi: 10.5455/aim.2013.21.129-134. http://europepmc.org/abstract/MED/24058254 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous