

Vitamin D and risk of pregnancy related hypertensive disorders: mendelian randomisation study
- PMID: 29925546
- PMCID: PMC6008987
- DOI: 10.1136/bmj.k2167
Vitamin D and risk of pregnancy related hypertensive disorders: mendelian randomisation study
Abstract
Objective: To use mendelian randomisation to investigate whether 25-hydroxyvitamin D concentration has a causal effect on gestational hypertension or pre-eclampsia.
Design: One and two sample mendelian randomisation analyses.
Setting: Two European pregnancy cohorts (Avon Longitudinal Study of Parents and Children, and Generation R Study), and two case-control studies (subgroup nested within the Norwegian Mother and Child Cohort Study, and the UK Genetics of Pre-eclampsia Study).
Participants: 7389 women in a one sample mendelian randomisation analysis (751 with gestational hypertension and 135 with pre-eclampsia), and 3388 pre-eclampsia cases and 6059 controls in a two sample mendelian randomisation analysis.
Exposures: Single nucleotide polymorphisms in genes associated with vitamin D synthesis (rs10741657 and rs12785878) and metabolism (rs6013897 and rs2282679) were used as instrumental variables.
Main outcome measures: Gestational hypertension and pre-eclampsia defined according to the International Society for the Study of Hypertension in Pregnancy.
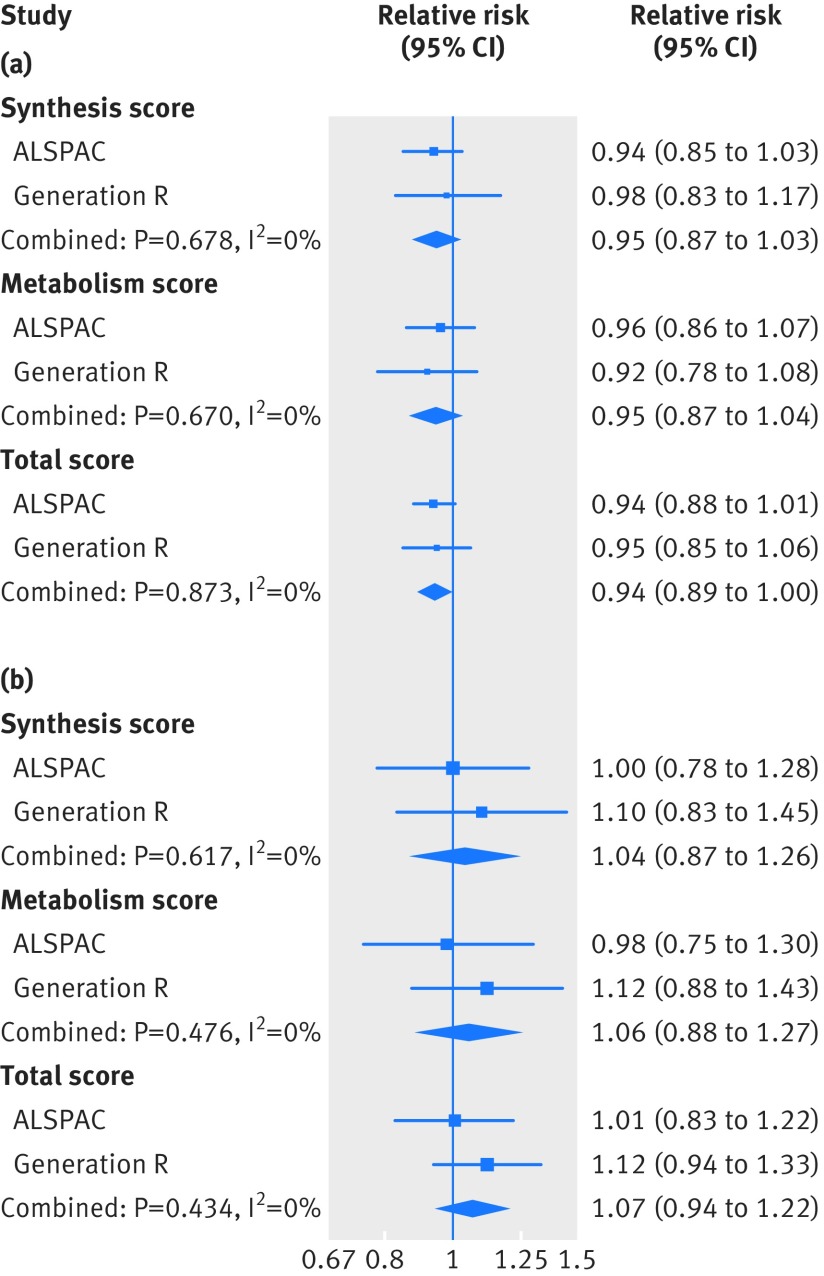
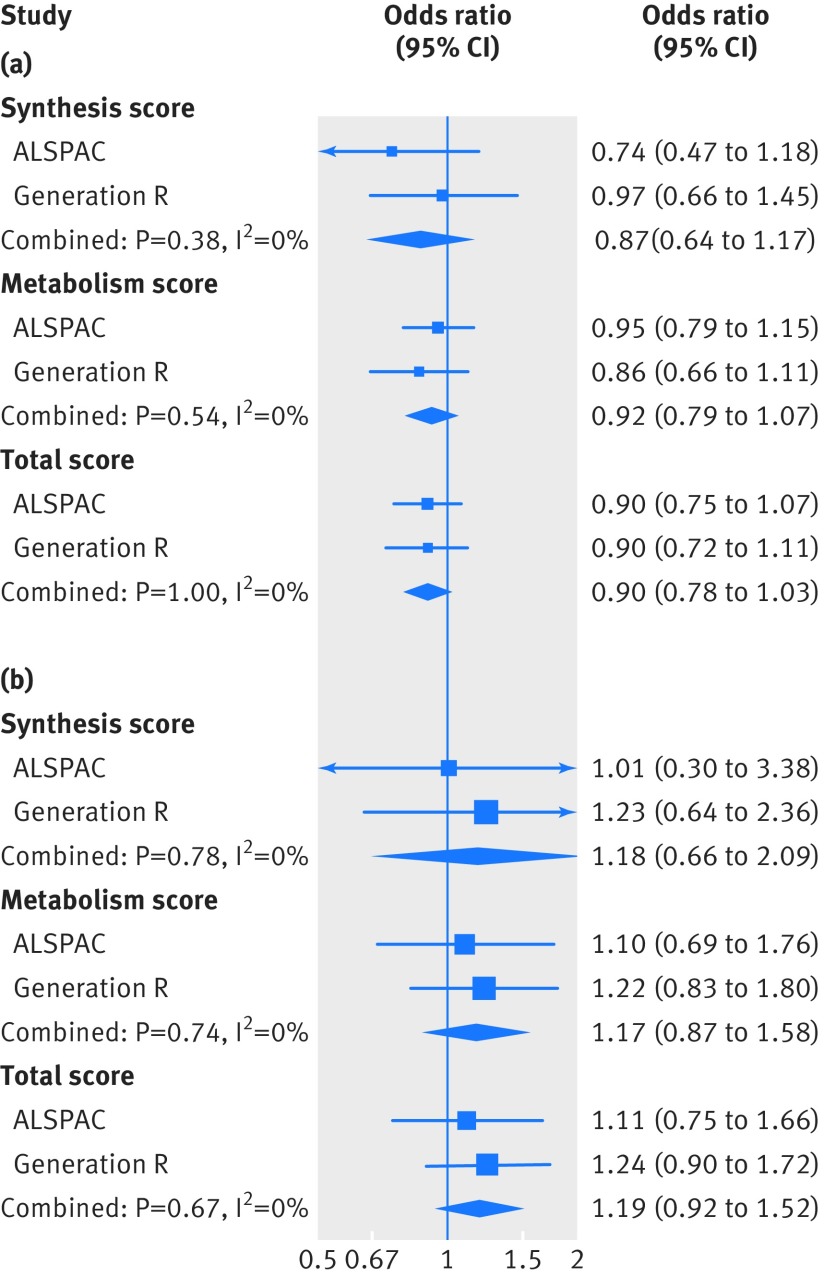
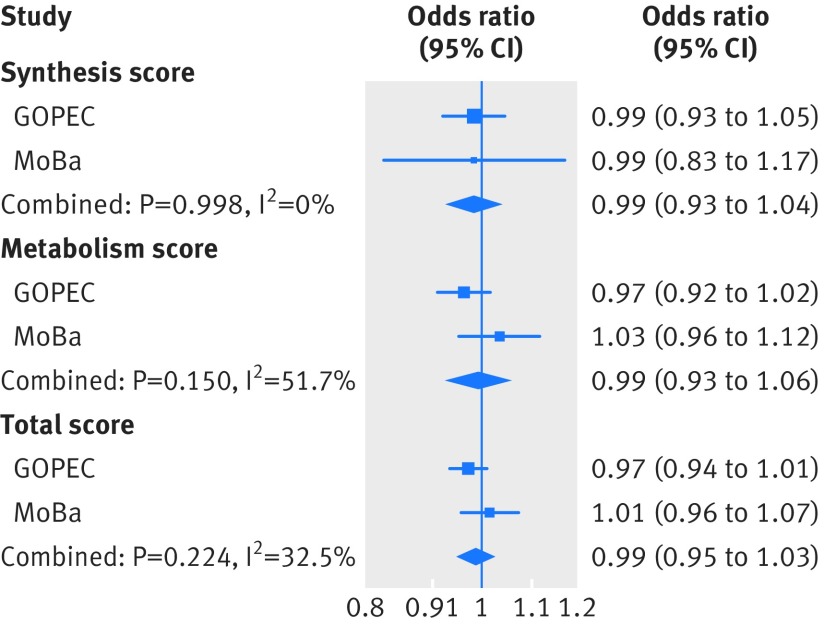
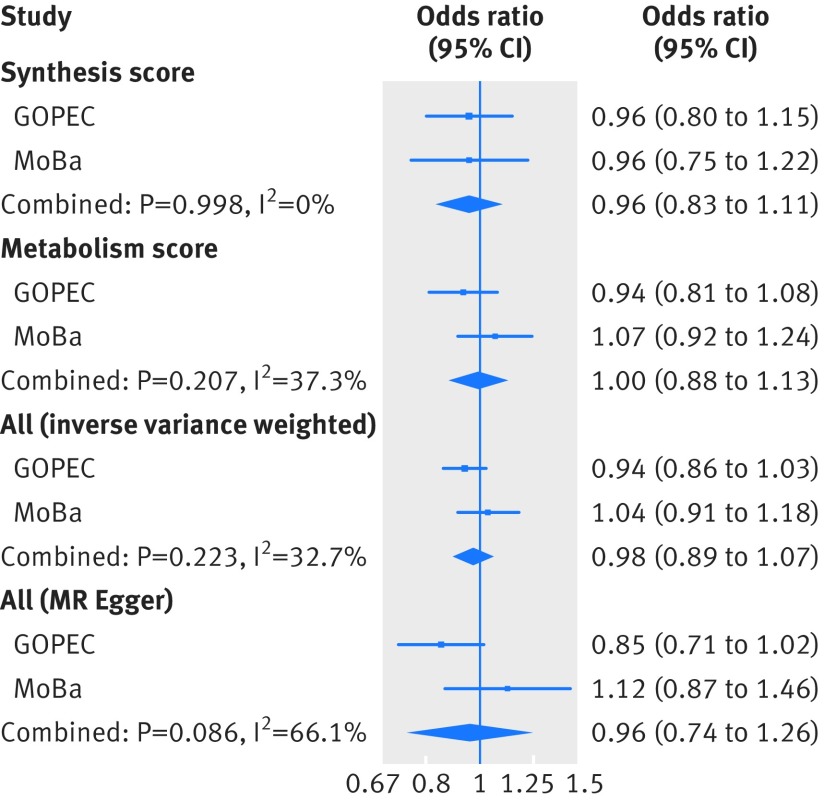
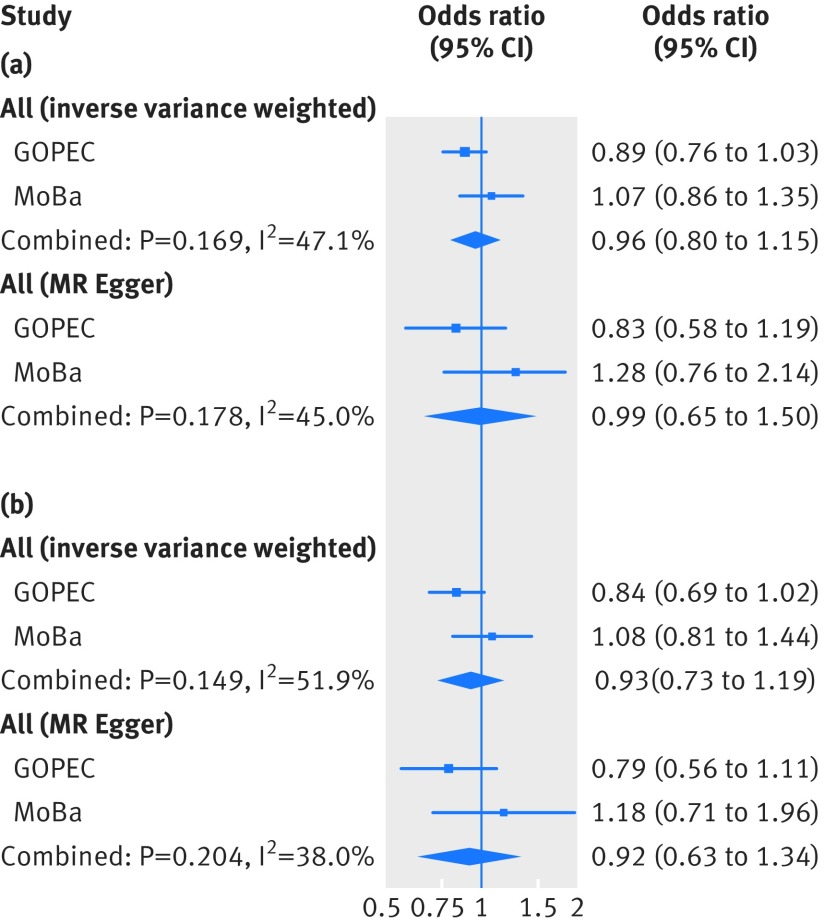
Results: In the conventional multivariable analysis, the relative risk for pre-eclampsia was 1.03 (95% confidence interval 1.00 to 1.07) per 10% decrease in 25-hydroxyvitamin D level, and 2.04 (1.02 to 4.07) for 25-hydroxyvitamin D levels <25 nmol/L compared with ≥75 nmol/L. No association was found for gestational hypertension. The one sample mendelian randomisation analysis using the total genetic risk score as an instrument did not provide strong evidence of a linear effect of 25-hydroxyvitamin D on the risk of gestational hypertension or pre-eclampsia: odds ratio 0.90 (95% confidence interval 0.78 to 1.03) and 1.19 (0.92 to 1.52) per 10% decrease, respectively. The two sample mendelian randomisation estimate gave an odds ratio for pre-eclampsia of 0.98 (0.89 to 1.07) per 10% decrease in 25-hydroxyvitamin D level, an odds ratio of 0.96 (0.80 to 1.15) per unit increase in the log(odds) of 25-hydroxyvitamin D level <75 nmol/L, and an odds ratio of 0.93 (0.73 to 1.19) per unit increase in the log(odds) of 25-hydroxyvitamin D levels <50 nmol/L.
Conclusions: No strong evidence was found to support a causal effect of vitamin D status on gestational hypertension or pre-eclampsia. Future mendelian randomisation studies with a larger number of women with pre-eclampsia or more genetic instruments that would increase the proportion of 25-hydroxyvitamin D levels explained by the instrument are needed.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and have the following declarations. MCM, AF, CB and DAL work at the Medical Research Council Integrative Epidemiology Unit at the University of Bristol which receives infrastructure funding from the UK MRC (MC/UU/12013/5). The contribution of AF and DAL were supported by the National Institute for Health Research Biomedical Research Centre at University Hospitals Bristol National Health Service Foundation Trust and the University of Bristol. MCM and AF are also supported by a UK MRC fellowship (MR/M009351/1) awarded to AF. DAL is also supported by the US National Institutes of Health (NF-SI-0611-10196) and a European Research Council Advanced Grant (DevelopObese; 669545); DAL is an NIHR Senior Investigator (R01 DK10324). DAL also reports funding from Roche Diagnostics and Medtronic for biomarker research, outside the current work. KM is supported through Erasmus Mundus Western Balkans (ERAWEB), a project funded by the European Commission. VWVJ received a grant from the Netherlands Organisation for Health Research and Development (NWO, ZonMw-VIDI 016.136.361) and a European Research Council Consolidator Grant (ERC-2014-CoG-648916). AEB was supported in part by the NIH (NICHD T32 HD052468). SJL is supported by the Intramural Research Program of the NIH (NIEHS). AB and SE report that genotyping of one of the cohorts included in the study was financed by the US NIH. JF reports a research grant from the European Research Council’s Horizon 2020 scheme. The views expressed in this publication are those of the authors and not necessarily those of any of the funders or of the UK NHS or the Department of Health.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical